-
Preprocedural prognostic nutritional index predicts early gastrointestinal symptoms after percutaneous endoscopic gastrostomy or percutaneous radiologic gastrostomy in Korea: a retrospective cohort study
-
Yoonhong Kim
 , Jee Young Lee, Yeajin Moon, Seung Hun Lee, Kyung Won Seo, Ki Hyun Kim , Jee Young Lee, Yeajin Moon, Seung Hun Lee, Kyung Won Seo, Ki Hyun Kim
-
Ann Clin Nutr Metab 2025;17(3):196-202. Published online December 1, 2025
-
DOI: https://doi.org/10.15747/ACNM.25.0032
-
-
 Graphical Abstract Graphical Abstract
 Abstract Abstract
 PDF PDF
 - Purpose
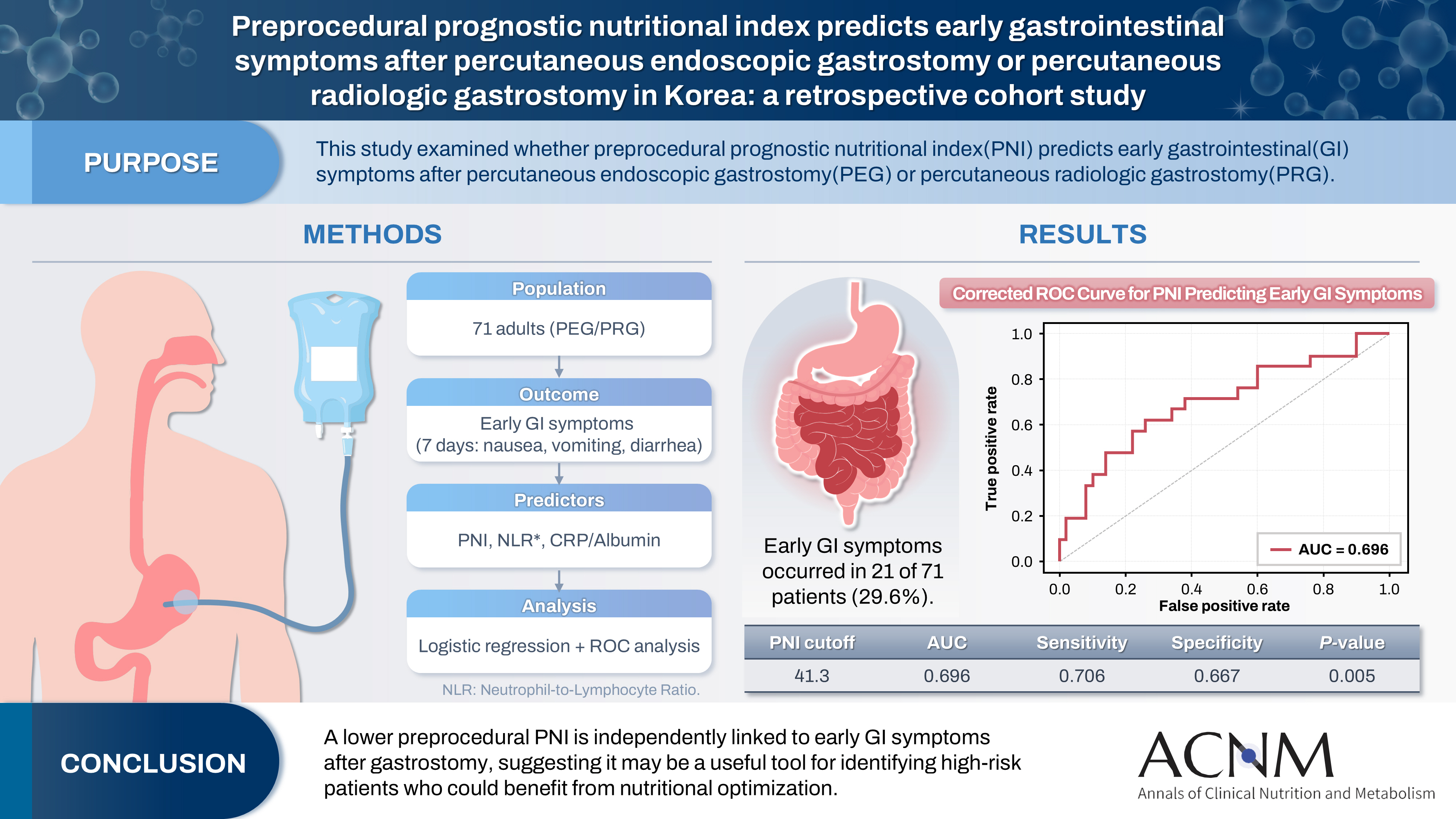
The prognostic nutritional index (PNI) reflects immunonutritional status and is a well-established predictor of surgical outcomes. Although its association with post-gastrostomy mortality has been documented, its relationship with early gastrointestinal (GI) symptoms remains unclear. This study aimed to evaluate whether the preprocedural PNI predicts early GI symptoms following percutaneous gastrostomy, including percutaneous endoscopic gastrostomy (PEG) and percutaneous radiologic gastrostomy (PRG).
Methods
This retrospective study included 71 adults who underwent PEG or PRG. Early GI symptoms, such as nausea, vomiting, and diarrhea, occurring within 7 days were recorded. The preprocedural PNI, neutrophil-to-lymphocyte ratio (NLR), and the C-reactive protein (CRP)-to-albumin ratio were analyzed using logistic regression to identify predictors. Receiver operating characteristic (ROC) analysis was performed to assess the PNI’s discriminative performance.
Results
Early GI symptoms occurred in 21 of 71 patients (29.6%). In univariate analysis, the PNI (P=0.009) and CRP-to-albumin ratio (P=0.018) were significant predictors, whereas NLR was not (P=0.125). After adjustment for potential confounders, including age, sex, body mass index, and NLR, the PNI remained an independent predictor of early GI symptoms (adjusted odds ratio, 0.90; 95% confidence interval, 0.83–0.98; P=0.021). ROC analysis for the PNI produced an area under the curve of 0.696, with an optimal cutoff value of 41.3 (sensitivity 70.6%, specificity 66.7%).
Conclusion
A lower preprocedural PNI is independently associated with the development of early GI symptoms after gastrostomy. The PNI may serve as a practical screening tool to identify high-risk patients who could benefit from preemptive nutritional optimization.
-
Citations
Citations to this article as recorded by  - Comment on “impact of percutaneous endoscopic gastrostomy (PEG) timing on mortality in intensive care unit patients: The modifying role of the prognostic nutritional index (PNI)”
M. Ganesan, K. Suresh Babu, K. Srinivasa Galu, Ponazhagan
Clinical Nutrition ESPEN.2026; 74: 103361. CrossRef
-
1,967
View
-
31
Download
-
1
Crossref
-
Nutritional support for critically ill patients by the Korean Society for Parenteral and Enteral Nutrition — part I: a clinical practice guideline
-
Seung Hwan Lee, Jae Gil Lee, Min Kwan Kwon, Jiyeon Kim, Mina Kim, Jeongyun Park, Jee Young Lee, Ye Won Sung, Bomi Kim, Seong Eun Kim, Ji Yoon Cho, A Young Lim, In Gyu Kwon, Miyoung Choi, KSPEN Guideline Committee
-
Ann Clin Nutr Metab 2024;16(3):89-111. Published online December 1, 2024
-
DOI: https://doi.org/10.15747/ACNM.2024.16.3.89
-
-
Abstract
PDF
 Supplementary Material Supplementary Material
- Purpose: Nutritional support for adult critically ill patients is essential due to the high risk of malnutrition, which can lead to severe complications. This paper aims to develop evidence-based guidelines to optimize nutritional support in intensive care units (ICUs).
Methods: The Grading Recommendations, Assessment, Development and Evaluation process was used to develop and summarize the evidence on which the recommendations were based. Clinical outcomes were assessed for seven key questions.
Results: We recommend the following: (1) initiate enteral nutrition (EN) within 48 hours after treatment as it is associated with improved outcomes, including reduced infection rates and shorter ICU stays; (2) early EN is preferred over early parenteral nutrition due to better clinical outcomes; (3) the use of supplementary parenteral nutrition to meet energy targets during the first week of ICU admission in patients receiving early EN is conditionally recommended based on patient-specific needs; (4) limited caloric support should be supplied to prevent overfeeding and related complications, particularly in the early phase of critical illness; (5) higher protein intake is suggested to improve clinical outcomes, such as muscle preservation and overall recovery; (6) additional enteral or parenteral glutamine is conditionally recommended against due to the lack of significant benefit and potential harm; and (7) fish oil-containing lipid emulsions is conditionally recommended due to their potential to enhance clinical outcomes, including reduced infection rates and shorter ICU stays.
Conclusion: These evidence-based recommendations can improve clinical outcomes and support healthcare providers in making informed decisions about nutritional interventions in the ICU.
-
Citations
Citations to this article as recorded by - Case Report: Optimizing wound care: tailored nutritional strategies with immune- modulating enteral nutrients
Fiji Antony, Wafaa Ayesh
Frontiers in Nutrition.2026;[Epub] CrossRef - Actualización en terapia médica nutricional del paciente críticamente enfermo: avances, desafíos y evidencia reciente
Nestor David Caicedo-Buitrago, Mateo Londoño-Pereira, Claudia Milena Ardila Melendez, Ricardo Merchán, Fernando Pereira-Paternina, Cristian Pinilla, Sonia Gamboa, Alejandra Cabral, Janeth Barbosa Barbosa, Maria del Pilar Morales, Bladimir Gil
Acta Colombiana de Cuidado Intensivo.2026; : 100612. CrossRef - Rationale for Determining Energy Requirement in Hospitalized Patients: A Narrative Review
Suk-Kyung Hong, Kyung Mo Kim
Pediatric Gastroenterology, Hepatology & Nutrition.2026; 29(3): 212. CrossRef - Early supplemental parenteral nutrition and risk of subsequent enteroatmospheric fistula in high-risk open abdomen patients with persistent enteral nutrition intolerance: a landmark propensity score-matched cohort study
Wenyue Wang, Tian Xie, Chen Chen, Fen Chen, Dongliang Yang, Pengfei Wang, Yousheng Li
Frontiers in Medicine.2026;[Epub] CrossRef - Development of a multidisciplinary cooperative nutrition management process for critically ill patients—a Delphi expert consensus study
Shunxia Sun, Jin Yang, Juan Huang, Jiangqiong Peng, Xiaoling Tang
Frontiers in Nutrition.2026;[Epub] CrossRef - Enteral Nutrition Versus a Combination of Enteral and Parenteral Nutrition in Critically Ill Adult Patients in the Intensive Care Unit: An Overview of Systematic Reviews and Meta-Analysis
Paraskevi Papanikolaou, Xenophon Theodoridis, Androniki Papaemmanouil, Niki N. Papageorgiou, Alexandra Tsankof, Anna-Bettina Haidich, Christos Savopoulos, Konstantinos Tziomalos
Journal of Clinical Medicine.2025; 14(3): 991. CrossRef
-
30,217
View
-
907
Download
-
6
Crossref
-
Association of early parenteral energy provision with serum phosphorus decline and phosphorus-based refeeding syndrome in critically ill patients with liver cirrhosis: a Korean retrospective observational study
-
Jee Young Lee, Yeo Kon Kye, Kwang Il Seo, Kyung Won Seo, SooYong Lee, Jesang Yu
-
Received May 7, 2026 Accepted June 30, 2026 Published online July 16, 2026
-
DOI: https://doi.org/10.15747/ACNM.26.0055
-
-
Abstract
- Background
Critically ill patients with liver cirrhosis are vulnerable to malnutrition and refeeding-related electrolyte disturbances, particularly when total parenteral nutrition is initiated with rapid caloric advancement. Because hypophosphatemia is a key biochemical feature of refeeding syndrome (RFS), and because phosphorus homeostasis may be impaired in cirrhosis, we evaluated the association of early parenteral energy provision with serum phosphorus changes, phosphorus-based RFS occurrence, and RFS severity in patients with cirrhosis admitted to the intensive care unit (ICU).
Methods
This retrospective observational study included 72 adults with liver cirrhosis who were admitted to the ICU of a tertiary referral hospital between January 2021 and August 2024. Parenteral energy intake was assessed on the day of emergency department (ED) presentation, ICU day 1, and ICU day 2. Serum phosphorus reduction was defined as the percentage decrease from the baseline value at ED presentation to the nadir within the first 5 ICU days. For this study, RFS was operationally defined using the serum phosphorus component of the 2020 American Society for Parenteral and Enteral Nutrition consensus recommendations: a ≥10% decrease in serum phosphorus within 5 days after reinitiating or substantially increasing energy provision was classified as phosphorus-based RFS, with severity categorized as mild (10%–20%), moderate (20%–30%), or severe (>30%). Potassium and magnesium were not used as independent diagnostic criteria because serial measurements were not consistently available for all patients. Renal replacement therapy, diuretic use, and phosphate supplementation were reviewed because these concurrent ICU interventions may directly affect serum phosphorus concentrations.
Results
A total of 72 critically ill patients with liver cirrhosis who were admitted to the ICU via the ED were analyzed; 53 patients (73.6%) met the phosphorus-based RFS criterion. These included eight patients (11.1%) with mild, 10 (13.9%) with moderate, and 35 (48.6%) with severe phosphorus-based RFS, categorized according to the magnitude of serum phosphorus decline. ICU day 2 caloric intake per body weight was positively correlated with the percentage reduction in serum phosphorus (r=0.346, R²=0.120, P=0.003). In multivariable linear regression analysis, both ED glucose load and ICU day 2 caloric intake per body weight were independently associated with greater serum phosphorus reduction (P=0.001 and P=0.011, respectively). Only ICU day 2 caloric intake per body weight remained independently associated with meeting the phosphorus-based RFS criterion (odds ratio, 1.19; 95% confidence interval, 1.06–1.36; P=0.007). Receiver operating characteristic curve analysis demonstrated fair but modest discriminative performance for ICU day 2 caloric intake per body weight in identifying phosphorus-based RFS status, with an area under the curve of 0.7061 and an exploratory cutoff of 10.92 kcal/kg/day.
Conclusion
In critically ill patients with liver cirrhosis, higher caloric delivery on ICU day 2 was associated with greater serum phosphorus decline and a higher likelihood of meeting the phosphorus-based RFS criterion within this cohort. These findings should be interpreted as exploratory associations rather than evidence of a causal effect of nutritional support on RFS development. The proposed ICU day 2 cutoff should be considered a hypothesis-generating observation requiring external validation. Careful monitoring of caloric delivery and serial electrolytes, including phosphate, potassium, and magnesium, may support safer parenteral nutrition in this population.
|
 E-submission
E-submission

