 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Funded articles
- Page Path
- HOME > Browse articles > Funded articles
Original Articles
- Postoperative nausea and vomiting after emergent abdominal surgery in trauma patients in Korea: a multicenter retrospective observational study
-
Doo-Hun Kim
 , Hoonsung Park, Heejin Kim, Jihyeon Ahn, Mina Choi, Dae-Sang Lee, Tae Hwa Hong, Hang Joo Cho, Maru Kim
, Hoonsung Park, Heejin Kim, Jihyeon Ahn, Mina Choi, Dae-Sang Lee, Tae Hwa Hong, Hang Joo Cho, Maru Kim - Ann Clin Nutr Metab 2026;18(2):138-144. Published online July 31, 2026
- DOI: https://doi.org/10.15747/ACNM.26.0044
- Funded: Korean Society of Surgical Metabolism and Nutrition
-
 Graphical Abstract
Graphical Abstract
 Abstract
Abstract
 PDF
PDF - Purpose
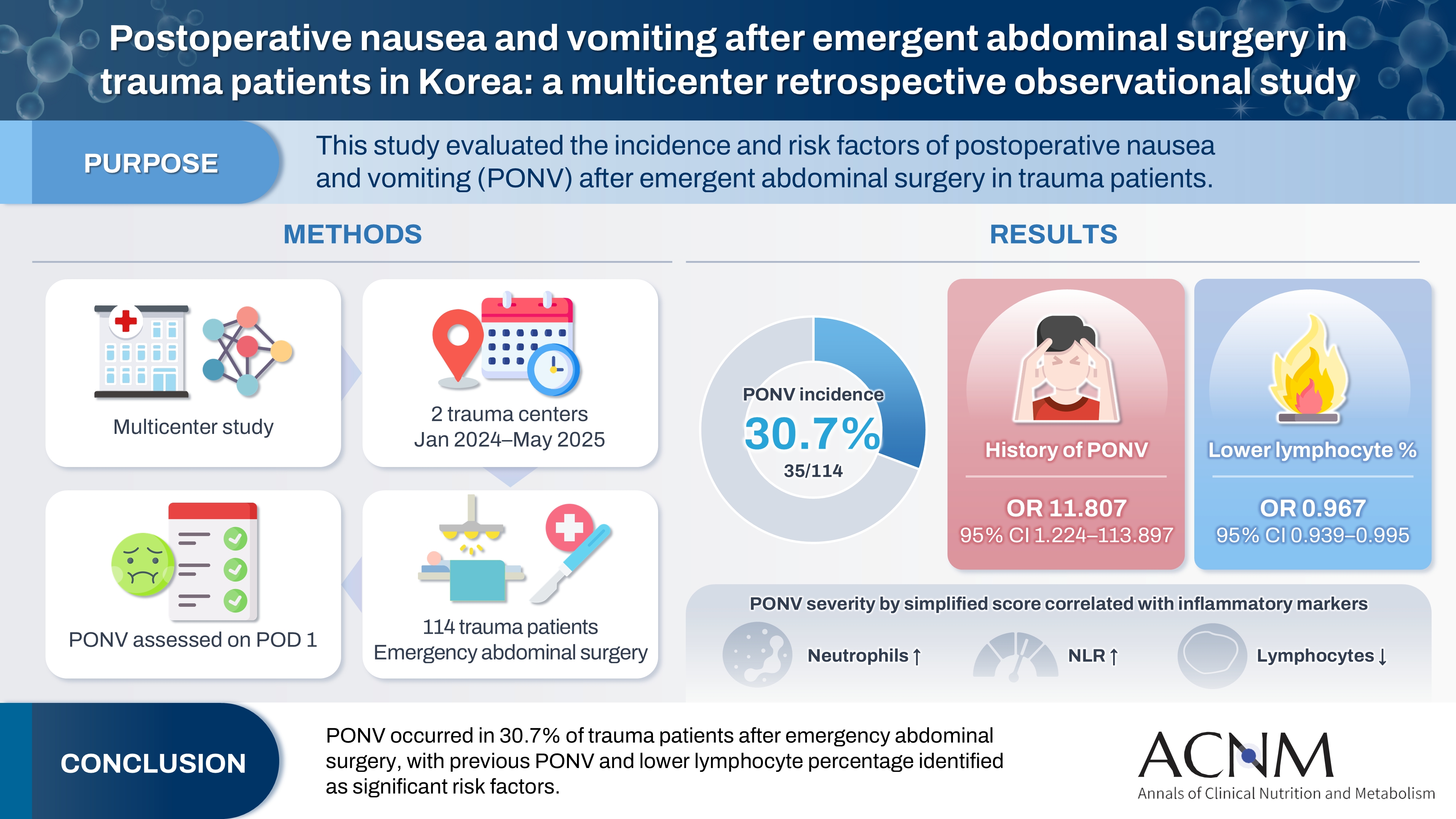
The present study aimed to assess the incidence and risk factors of postoperative nausea and vomiting (PONV) after emergency abdominal surgery in trauma patients.
Methods
This retrospective observational study included trauma patients who underwent emergency abdominal surgery at two trauma centers between January 2024 and May 2025. Medical records were reviewed according to the occurrence of PONV.
Results
A total of 114 patients were included in the analysis, of whom 35 patients (30.7%) developed PONV. Patients with a history of PONV had a higher incidence of PONV than those without such a history (80% vs. 28.4%; P=0.030). The lymphocyte percentage was lower in the PONV group (27.8% vs. 20.0%; P=0.023). In binary logistic regression analysis, previous PONV (B=2.469, P=0.033; odds ratio [OR], 11.807; 95% confidence interval [CI], 1.224–113.897) and lymphocyte percentage (B=−0.034, P=0.021; OR, 0.967; 95% CI, 0.939–0.995) were significant risk factors. PONV severity was also associated with a higher segmented neutrophil percentage, a higher neutrophil-to-lymphocyte ratio, and a lower lymphocyte percentage.
Conclusion
The incidence of PONV was 30.7%. Previous PONV and a lower lymphocyte percentage were identified as risk factors for PONV after emergency abdominal surgery in trauma patients. Further studies are needed to develop strategies for reducing PONV in this population.
- 150 View
- 7 Download

- Epigallocatechin gallate increases fatty acid oxidation but not 24-hour survival in lipopolysaccharide-induced endotoxic shock in mice
-
Takayuki Irahara
 , Ryusuke Katsuki, Dai Oishi, Tsuguaki Terashima, Md. Monirul Islam
, Ryusuke Katsuki, Dai Oishi, Tsuguaki Terashima, Md. Monirul Islam , Umme Salma, Shohag Majumder, Ridwan Ahmed, Eizo Watanabe
, Umme Salma, Shohag Majumder, Ridwan Ahmed, Eizo Watanabe - Ann Clin Nutr Metab 2026;18(1):27-33. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0036
- Funded: Japan Society for the Promotion of Science
-
Graphical Abstract
Abstract
PDF
- Purpose
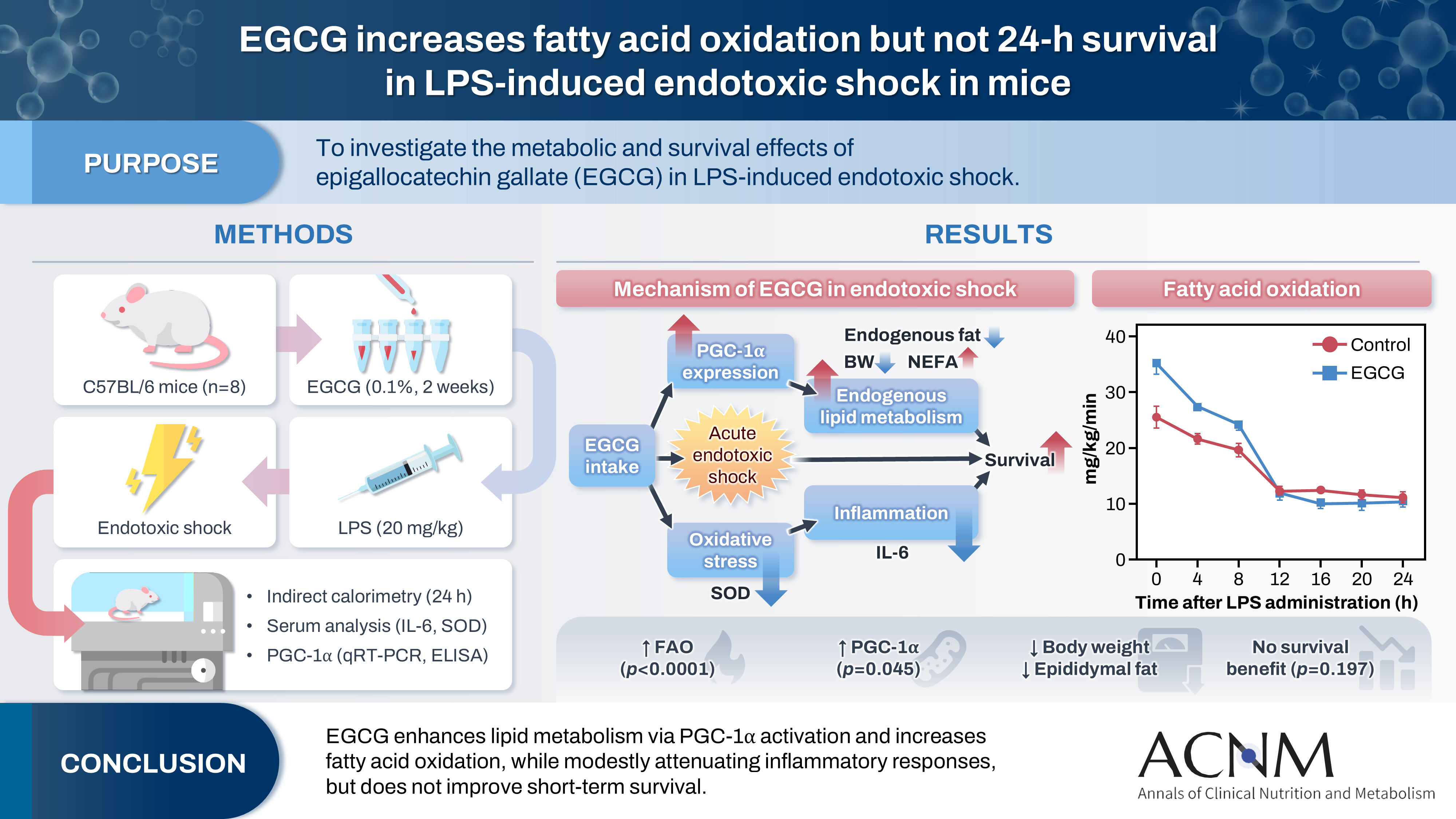
This study aimed to explore the effects of epigallocatechin gallate (EGCG) in critically ill patients using a mouse model.
Methods
C57BL/6 mice were divided into control and EGCG groups (n=8 per group). The EGCG group received a 0.1% EGCG solution for 2 weeks, after which the mice were intraperitoneally injected with a lethal dose of lipopolysaccharide to induce acute endotoxic shock. Indirect calorimetry was performed for 24 hours. Changes in body weight, epididymal fat weight, and survival were measured, together with serum lipid levels, interleukin-6 (IL-6), and superoxide dismutase (SOD) concentrations. The expression of peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α) was determined using quantitative real-time polymerase chain reaction, and its serum concentration was subsequently measured.
Results
Indirect calorimetry showed a significant increase in fatty acid oxidation (P<0.0001) in the EGCG group, along with significant decreases in body weight and epididymal fat weight (P<0.01 and P<0.05, respectively). Survival did not differ significantly between groups (P=0.197). Serum lipid levels, IL-6, and SOD showed numerical differences, although these differences were not statistically significant. Furthermore, hepatic PGC-1α expression showed a tendency toward upregulation, and serum PGC-1α levels were significantly higher (P<0.05).
Conclusion
EGCG stimulates endogenous lipid metabolism through PGC-1α activation and may suppress inflammatory responses; therefore, it may represent a potentially useful nutrient for acute nutritional therapy.
- 3,209 View
- 38 Download
Guideline
- A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part III. preparation of enteral nutrition formulas
-
In Seok Lee, Ye Rim Chang, Bo-Eun Kim, Youn Soo Cho, Sung-Sik Han, Eunjung Kim, Hyunjung Kim, Jae Hak Kim, Jeong Wook Kim, Sung Shin Kim, Eunhee Kong, Ja Kyung Min, Chi-Min Park, Jeongyun Park, Seungwan Ryu, Kyung Won Seo, Jung Mi Song, Minji Seok, Eun-Mi Seol, Jinhee Yoon, Jeong-Meen Seo, for the KSPEN Enteral Nutrition Committee
- Ann Clin Nutr Metab 2026;18(1):3-9. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.26.0046
- Funded: Korean Society for Parenteral and Enteral Nutrition
-
Abstract
PDF
- Purpose
This guideline was developed to provide evidence-based recommendations for the safe preparation and handling of enteral nutrition (EN) formulas in order to improve patient safety and promote standardized clinical practice in Korea.
Methods
The key questions addressed the selection of open versus closed feeding systems, the safe preparation and handling of EN formulas, precautions related to blenderized tube feeding (BTF), and essential labeling requirements. Recommendations were drafted and refined through multidisciplinary expert consensus under the auspices of the Korean Society for Parenteral and Enteral Nutrition (KSPEN).
Results
The choice of feeding system should be determined according to the patient’s condition, risk of infection, and anticipated duration of feeding. Closed feeding systems are recommended because they reduce contamination risk and nursing workload, whereas open feeding systems require strict adherence to aseptic technique. For open or reconstituted EN formulas, hang time at room temperature should not exceed 4 hours, whereas closed feeding systems should follow the manufacturer’s recommended hang time. For BTF, administration time should be limited to 2 hours to minimize bacterial growth, and their use is contraindicated in medically unstable or immunocompromised patients. Accurate labeling, including patient identifiers, formula information, administration route, and hang time, is essential to prevent administration errors.
Conclusion
These guidelines provide a practical framework for the safe preparation and management of EN formulas. Adherence to standardized preparation protocols, including appropriate feeding system selection and strict hygiene practices, is essential for reducing complications and improving the safety of EN therapy.
- 2,777 View
- 88 Download
Original Article
- Perioperative nutritional practices and pediatric nutrition support team implementation in Korea: a cross-sectional study
-
Dayoung Ko, Honam Hwang, Hee-Beom Yang, Joong Kee Youn, Hyun-Young Kim
- Ann Clin Nutr Metab 2025;17(3):181-187. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0027
- Funded: Korean Society of Surgical Metabolism and Nutrition
-
Graphical Abstract
Abstract
PDF
 Supplementary Material
Supplementary Material - Purpose
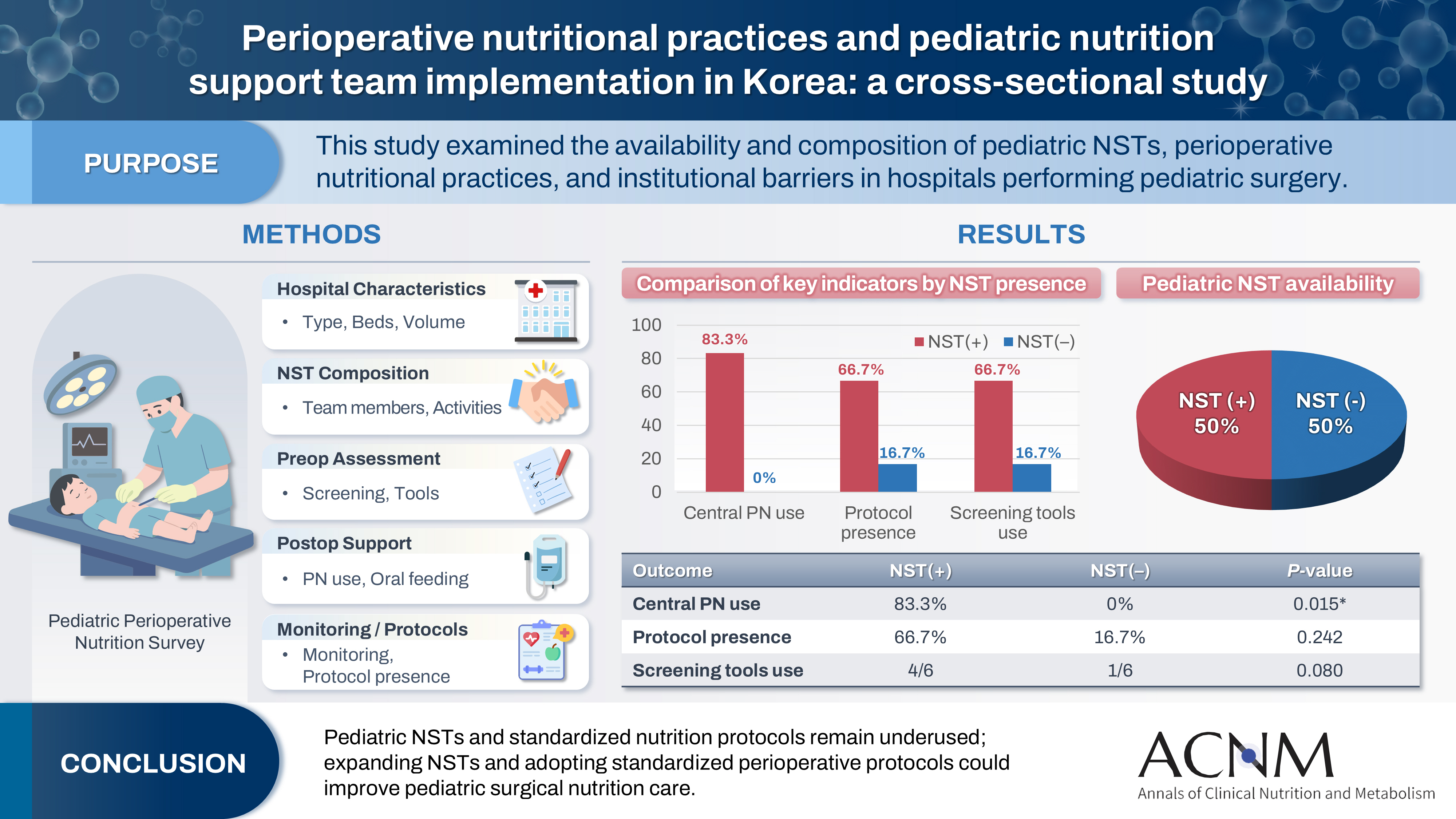
Pediatric surgical patients are vulnerable to perioperative malnutrition, yet standardized nutritional care and structured nutrition support team (NST) involvement remain inconsistent across institutions. Although multidisciplinary nutritional support has gained increasing attention, data on pediatric NST practices within surgical settings in Korea are limited. This study examined the availability and composition of pediatric NSTs, perioperative nutritional practices, and barriers in hospitals performing pediatric surgery.
Methods
A nationwide cross-sectional survey was conducted among tertiary and secondary hospitals that perform pediatric surgery in Korea. The questionnaire assessed hospital characteristics, the presence and composition of pediatric NSTs, perioperative nutritional screening and support practices, monitoring protocols.
Results
A total of 12 hospitals participated. Although all were high-capacity institutions, only half reported having a pediatric NST. Routine preoperative nutritional screening was performed in 50% of hospitals, and validated tools such as Screening Tool for the Assessment of Malnutrition in Pediatrics (STAMP) and Pediatric Yorkhill Malnutrition Score (PYMS) were used in 41.7%. Hospitals with a pediatric NST more frequently had institutional protocols for nutritional evaluation (66.7% vs. 16.7%) and were more likely to administer central venous parenteral nutrition postoperatively (83.3% vs. 0%, P=0.015). Enhanced Recovery After Surgery protocols were implemented in only two hospitals (16.7%). Major barriers to pediatric NST operation included insufficient staffing and time constraints.
Conclusion
Pediatric NSTs and standardized perioperative nutrition protocols remain underutilized in Korean surgical centers. Institutions with a pediatric NST demonstrated more structured nutritional practices. Expanding NST infrastructure and establishing standardized perioperative protocols for pediatric surgical patients may enhance the quality and consistency of nutritional care.
- 2,662 View
- 44 Download
Guideline
- The 2024 Korean Enhanced Recovery After Surgery guidelines for hepatobiliary and pancreatic surgery
-
Kwangpyo Hong, Hongbeom Kim, Hyung Sun Kim, Hae Won Lee, Ho Joong Choi, YoungRok Choi, Jae Do Yang, Sung-Moon Jeong, Dae Wook Hwang, Do Joong Park, Sang-Jae Park, The Korean Enhanced Recovery After Surgery (ERAS) Committee within the Korean Society of Surgical Metabolism and Nutrition
- Ann Clin Nutr Metab 2025;17(3):172-180. Published online December 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0034
- Funded: National Cancer Center
-
Abstract
PDF
- Purpose
The Korean Enhanced Recovery After Surgery (ERAS) Committee within the Korean Society of Surgical Metabolism and Nutrition has developed comprehensive guidelines for hepatobiliary and pancreatic (HBP) surgery by adapting established international protocols. These guidelines provide evidence-based recommendations specifically tailored to the Korean healthcare system and address perioperative management for both pancreatoduodenectomy and hepatectomy.
Methods
The HBP subcommittee reviewed existing international ERAS guidelines and conducted an adaptation process. Key questions were identified based on national survey results from Korean HBP surgeons and were prioritized according to clinical relevance. The committee focused on elements supported by moderate- to high-quality evidence with strong recommendation grades. Literature searches were conducted through January 2025, and evidence quality was evaluated using GRADE methodology. Four key questions underwent formal assessment, and eight additional questions were adapted from international guidelines.
Results
Twelve key questions were selected and addressed, covering critical perioperative care domains: prehabilitation, preoperative nutritional assessment and support, anti-thrombotic prophylaxis, prophylactic abdominal drainage, preoperative biliary drainage, smoking and alcohol cessation, pre-anesthetic medication, minimally invasive surgical approaches, prophylactic nasogastric intubation, postoperative glycemic control, perianastomotic drainage management, and early mobilization protocols. Each recommendation was assigned specific evidence levels and graded for strength. High-quality evidence supported strong recommendations for the routine avoidance of prophylactic drainage in uncomplicated hepatectomy, early drain removal after pancreatoduodenectomy in low-risk patients, elimination of routine nasogastric decompression, and the implementation of early mobilization strategies.
Conclusion
These Korean-adapted ERAS guidelines for HBP surgery are expected to standardize perioperative care, reduce postoperative complications, shorten hospital stays, and enhance overall patient outcomes across Korean healthcare institutions. -
Citations
Citations to this article as recorded by
- Adapting Enhanced Recovery After Surgery for hepatobiliary and pancreatic surgery: a Korean perspective
Sang Hyun Shin
Ann Clin Nutr Metab.2026; 18(1): 1. CrossRef - Comparative evaluation of immediate outcomes of ERAS-associated and traditional postoperative management after pancreatic resection
J. A. Abdullozoda, Y. F. Tagoymurodov, A. I. Murodzoda, S. G. Ali-Zade
Health care of Tajikistan.2026; (2): 11. CrossRef
- Adapting Enhanced Recovery After Surgery for hepatobiliary and pancreatic surgery: a Korean perspective
- 4,450 View
- 106 Download
- 2 Crossref
Original Articles
- Insulinotropic action of L-carnitine and branched-chain amino acids following energy intake in healthy, young Japanese women: a non-randomized controlled trial
-
Yoichi Sakurai, Hideyuki Namba, Satoshi Odo
- Ann Clin Nutr Metab 2025;17(2):139-148. Published online August 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0011
- Funded: Ministry of Education, Culture, Sports, Science and Technology, Grant-inAid for Scientific Research
-
Abstract
PDF
- Purpose
The present study uses healthy human volunteers to examine the insulinotropic action of L-carnitine and branched-chain amino acids (BCAAs) after energy intake.
Methods
A total of 39 young, healthy human volunteers were assigned to receive oral doses of either L-carnitine alone (L group, n=10) or L-carnitine combined with a single or long-term continuous dose of BCAAs. Controls (C group, n=16) received none of these. L-carnitine was administered orally at 1,000 mg/d for 14 days, and BCAA was administered orally either once just before exercise (L+SB group, n=6), or every day for 14 days (L+CB group, n=7) until 2 days before the experiment. After overnight fasting, 200 kcal of glucose and oral nutritional supplement were administered to prevent hypoglycemia. Blood glucose, free-fatty acid, and serum insulin levels were measured to examine the insulinotropic action before and after exercise.
Results
Blood glucose and serum insulin levels in the L group were significantly lower than those in the C group. While the serum insulin levels were higher after energy administration than those in the fasting state in all groups, these were significantly higher in the L+SB group and in the L+CB group compared with those in the L group. The insulinotropic action after energy intake remained even after the repeated administration of BCAA discontinued 2 days before the experi¬ment and even after serum BCAA levels remained the same.
Conclusion
While the insulinotropic action appeared after a single dose of BCAA, it was also potentiated by long-term repeated oral administration of BCAA.
- 3,145 View
- 16 Download
- Development of a Japanese version of the Short Bowel Syndrome-Quality of Life (SBS-QoL) scale
-
Yuko Tazuke, Mayu Suzuki, Sae Kikuchi, Kaori Ishiguro, Hiroomi Okuyama
- Ann Clin Nutr Metab 2025;17(2):132-138. Published online August 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0016
- Funded: Takeda Pharmaceutical Company Limited
-
Graphical Abstract
Abstract
PDF
- Purpose
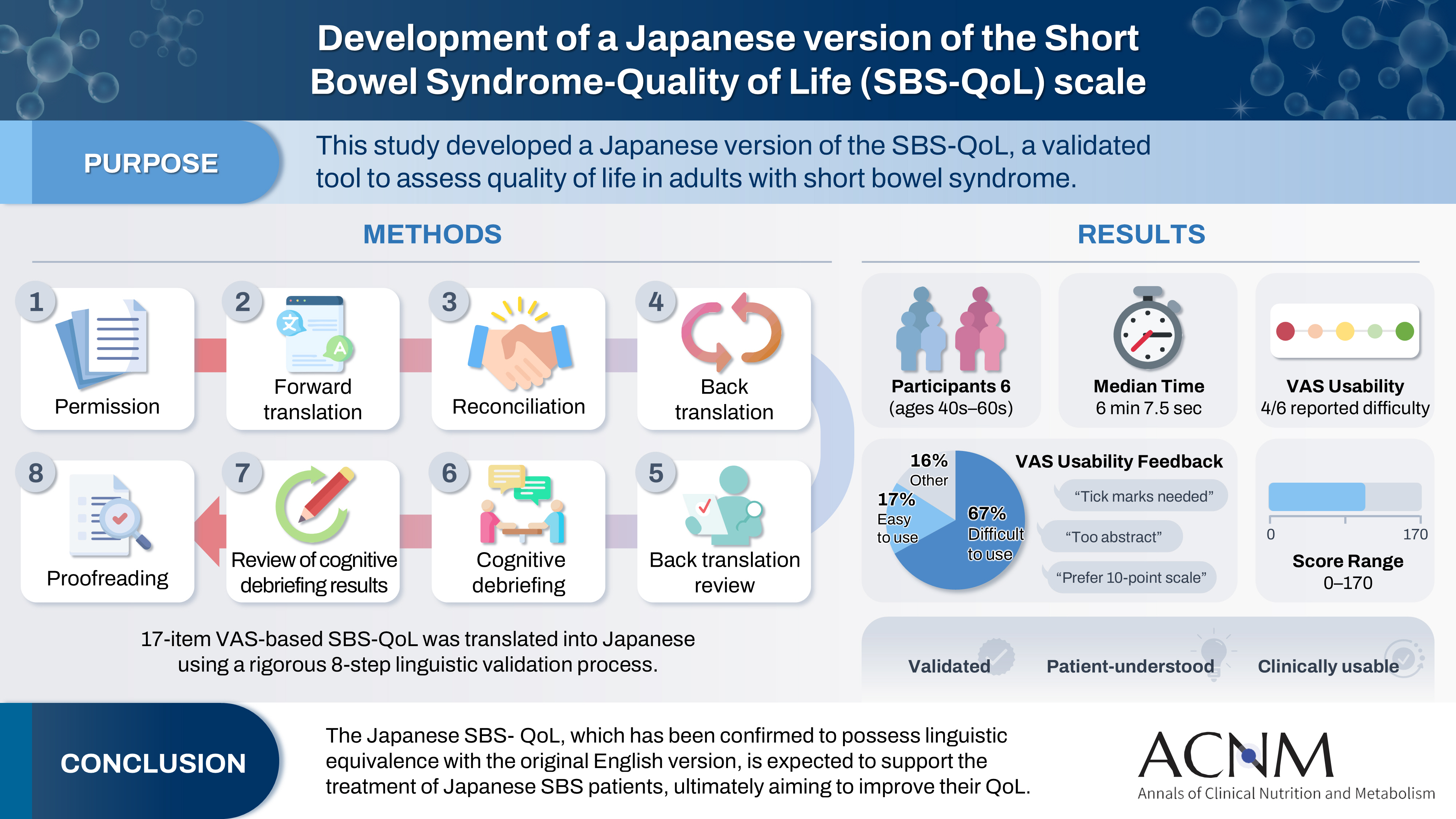
The Short Bowel Syndrome‐Quality of Life (SBS‐QoL) scale is a reliable and sensitive instrument developed to measure and evaluate the quality of life (QoL) in adult patients with short bowel syndrome (SBS). In Japan, increasing attention has been given to the assessment of QoL in patients with SBS; however, no Japanese‐language SBS‐specific scale is currently available. This study aimed to develop a Japanese version of the SBS‐QoL based on the original English version.
Methods
A provisional Japanese version was created in accordance with the guidelines of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) Task Force, utilizing a process of forward translation, adjustment, and back translation.
Results
Cognitive debriefing using the provisional Japanese version was conducted with six Japanese patients with SBS. Based on these results, the Japanese wording was evaluated and revised, leading to the creation of the final Japanese version.
Conclusion
The Japanese SBS‐QoL, which has been confirmed to possess linguistic equivalence with the original English version, is expected to support the treatment of Japanese SBS patients, ultimately aiming to improve their QoL.
- 5,283 View
- 33 Download
- Evaluation of the modified Nutrition Risk in Critically Ill score in Korean critically ill patients with COVID-19: a retrospective cohort study
-
Won Ho Han, Jong-Mog Lee, Jae Hoon Lee, Hyun Mi Lee, Ji-Yeon Kim, Mok Young Jang, Sung-Sik Han
- Ann Clin Nutr Metab 2025;17(2):125-131. Published online August 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0009
- Funded: National Cancer Center
-
Abstract
PDFSupplementary Material
- Purpose
We evaluated the efficacy of the modified Nutrition Risk in Critically Ill (mNUTRIC) score for malnutrition screening and its association with mortality in intensive care unit (ICU) patients with COVID-19.
Methods
The nutritional status of 129 COVID-19 ICU patients admitted between February 2021 and May 2022 was assessed using American Society for Parenteral and Enteral Nutrition/Academy of Nutrition and Dietetics (ASPEN/AND) criteria. The sensitivity, specificity, and clinical correlations of the mNUTRIC score were analyzed.
Results
Of the 129 patients, 35 (27.1%) met the ASPEN/AND malnutrition criteria. Multivariable analysis identified the mNUTRIC score, underlying malignancy, and mechanical ventilation as significant factors associated with malnutrition. The mNUTRIC score had a sensitivity of 77.1% and specificity of 63.8% (area under the curve [AUC], 0.71; 95% confidence interval [CI], 0.62–0.79) for diagnosing malnutrition, improving to 88.6% and 80.9%, respectively, after adjusting for malignancy and ventilation (AUC, 0.89; 95% CI, 0.82–0.95). Patients with a low mNUTRIC score had a mortality rate of 2.9% and a median ICU stay of 7.7 days (range, 0–84.2 days), whereas those with a high score (≥5) had a mortality rate of 13.1% and a median ICU stay of 10.2 days (range, 1.4–88.5 days) (P=0.046 and P=0.011, respectively).
Conclusion
The mNUTRIC score is an effective screening tool for malnutrition in ICU patients with COVID-19, especially those with malignancy or requiring mechanical ventilation, and is strongly associated with mortality and length of ICU stay.
- 4,743 View
- 41 Download
- Development of a pre- and re-habilitation protocol for gastrointestinal cancer surgery
-
Eun Young Kim, Jung Hoon Bae, Jiseon Kim, Eun Joo Yang, Sang-Jae Park, In Kyu Lee, on behalf of the Task Force Team for Development and Trial Application of Pre/Rehabilitation Protocol in GI Cancer Surgery
- Ann Clin Nutr Metab 2025;17(1):25-40. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0001
- Funded: Korean Society of Surgical Metabolism and Nutrition
-
Abstract
PDFSupplementary Material
- Purpose
Surgical resection is the primary curative treatment for gastrointestinal (GI) cancer; however, it is associated with high postoperative complication rates and impaired recovery. Frailty, malnutrition, and sarcopenia increase morbidity and mortality, underscoring the need for perioperative rehabilitation programs. Standardized rehabilitation protocols during the perioperative period are currently lacking in Korea. We aimed to develop an evidence-based rehabilitation protocol for GI cancer patients to enhance postoperative outcomes and facilitate clinical implementation.
Methods
A multidisciplinary task force team comprising experts in surgery, clinical nutrition, and rehabilitation medicine conducted a systematic literature search and comprehensive review from 2012 to 2022 to develop a standardized pre- and re-habilitation protocol for GI cancer surgery. The protocol underwent external validation and subsequent refinements before being finalized through expert consensus.
Results
The protocol development process was organized into four consecutive phases: keyword selection, literature review and case report form development, initial protocol drafting, and external validation leading to the final version of the protocol. The final version of the rehabilitation protocol is presented in the main text and included as Supplements.
Conclusion
This protocol provides a standardized clinical guideline based on the latest evidence-based pre- and re-habilitation strategies and is designed for seamless integration into routine clinical practice. By facilitating proactive rehabilitation interventions, it aims to improve outcomes in GI cancer patients who are at high risk of postoperative complications, functional decline, and malnutrition.
- 5,819 View
- 148 Download
 First
First Prev
Prev

