 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Search
- Page Path
- HOME > Search
Original Articles
- Current status and short-term results regarding frailty in patients undergoing gastrointestinal cancer resection in Japan: a retrospective cohort study
-
Asuka Yasueda
 , Junichi Nishimura, Seiji Ikeda, Naotsugu Haraguchi, Hirofumi Akita, Hiroshi Wada, Chu Matsuda, Takeshi Omori, Masayoshi Yasui, Hironari Tamiya, Hideaki Tahara, Hiroshi Miyata
, Junichi Nishimura, Seiji Ikeda, Naotsugu Haraguchi, Hirofumi Akita, Hiroshi Wada, Chu Matsuda, Takeshi Omori, Masayoshi Yasui, Hironari Tamiya, Hideaki Tahara, Hiroshi Miyata - Ann Clin Nutr Metab 2026;18(1):54-62. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0013
-
 Graphical Abstract
Graphical Abstract
 Abstract
Abstract
 PDF
PDF - Purpose
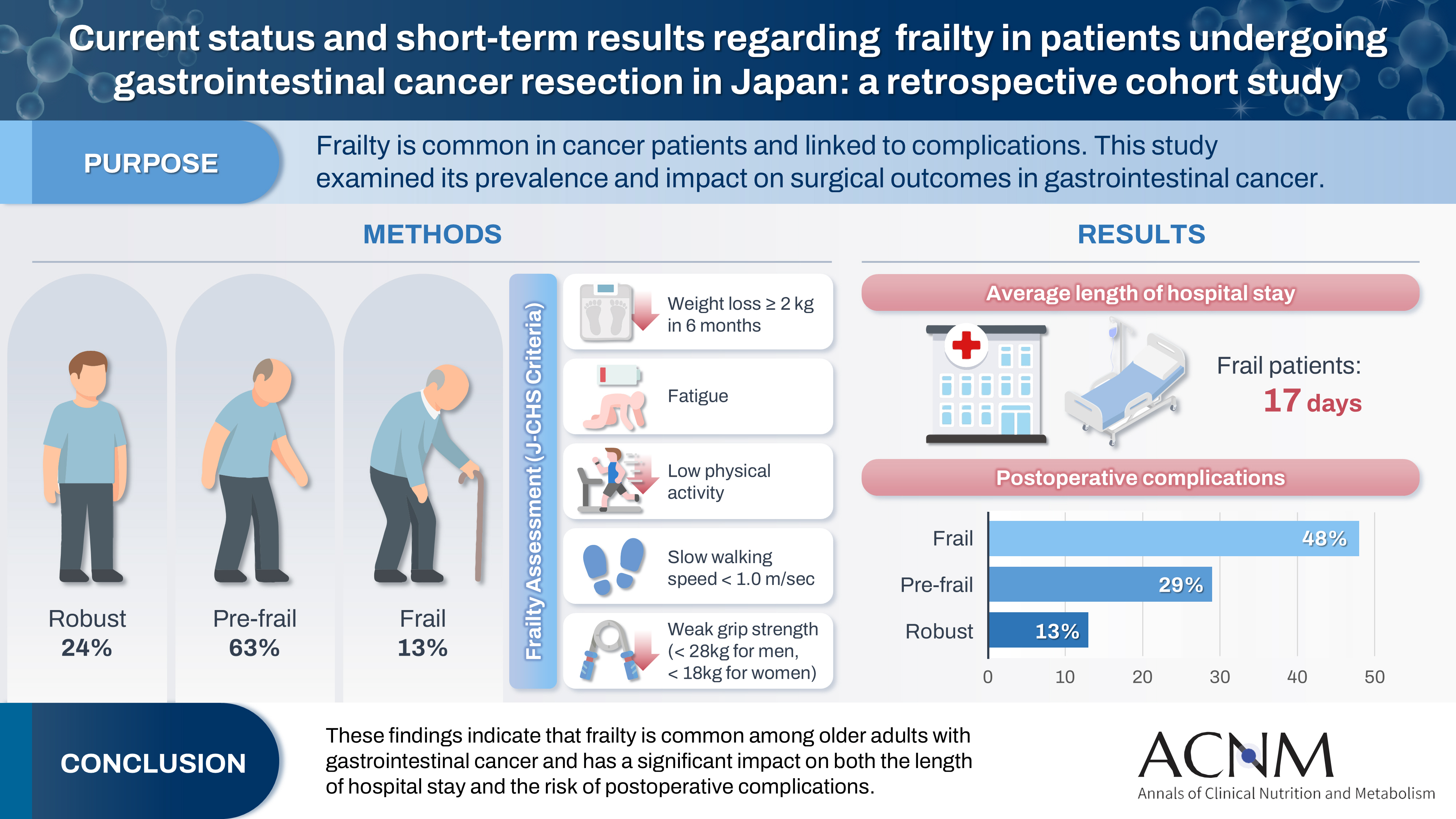
Frailty is a state of physical and cognitive decline that exists between robust health and the need for nursing care. Frailty is reported to occur at a high rate among patients with cancer and is associated with postoperative complications, such as delirium, infection, reduced survival, and rehospitalization. In this study, we investigated the incidence of frailty and surgical outcomes in patients who underwent surgery for gastrointestinal cancer.
Methods
A total of 201 patients who underwent preoperative physical assessment at Osaka International Cancer Institute between July and September 2021 were included. The Japanese version of the Cardiovascular Health Study (J-CHS) index was used to assess the frequency of frailty and related postoperative outcomes.
Results
Among the 201 patients, 27 (13%) were classified as frail and 126 (63%) as pre-frail. Of the 27 frail patients, 22 (81%) were older adults—a significantly higher proportion compared to the pre-frail/robust group (P=0.004). The median hospital stay for frail patients was 17 days (range, 5–98 days), which was significantly longer than that for robust patients (P<0.001). Postoperative complications occurred in 13 frail patients (48%), which was higher than in pre-frail (n=36, 29%) and robust (n=6, 13%) patients. Furthermore, multivariate analysis showed that frailty was an independent risk factor for postoperative complications.
Conclusion
These findings indicate that frailty is common among older adults with gastrointestinal cancer and has a significant impact on both the length of hospital stay and the risk of postoperative complications.
- 860 View
- 11 Download

- Development of a pre- and re-habilitation protocol for gastrointestinal cancer surgery
-
Eun Young Kim
 , Jung Hoon Bae, Jiseon Kim, Eun Joo Yang, Sang-Jae Park, In Kyu Lee, on behalf of the Task Force Team for Development and Trial Application of Pre/Rehabilitation Protocol in GI Cancer Surgery
, Jung Hoon Bae, Jiseon Kim, Eun Joo Yang, Sang-Jae Park, In Kyu Lee, on behalf of the Task Force Team for Development and Trial Application of Pre/Rehabilitation Protocol in GI Cancer Surgery - Ann Clin Nutr Metab 2025;17(1):25-40. Published online April 1, 2025
- DOI: https://doi.org/10.15747/ACNM.25.0001
-
Abstract
PDF
 Supplementary Material
Supplementary Material - Purpose
Surgical resection is the primary curative treatment for gastrointestinal (GI) cancer; however, it is associated with high postoperative complication rates and impaired recovery. Frailty, malnutrition, and sarcopenia increase morbidity and mortality, underscoring the need for perioperative rehabilitation programs. Standardized rehabilitation protocols during the perioperative period are currently lacking in Korea. We aimed to develop an evidence-based rehabilitation protocol for GI cancer patients to enhance postoperative outcomes and facilitate clinical implementation.
Methods
A multidisciplinary task force team comprising experts in surgery, clinical nutrition, and rehabilitation medicine conducted a systematic literature search and comprehensive review from 2012 to 2022 to develop a standardized pre- and re-habilitation protocol for GI cancer surgery. The protocol underwent external validation and subsequent refinements before being finalized through expert consensus.
Results
The protocol development process was organized into four consecutive phases: keyword selection, literature review and case report form development, initial protocol drafting, and external validation leading to the final version of the protocol. The final version of the rehabilitation protocol is presented in the main text and included as Supplements.
Conclusion
This protocol provides a standardized clinical guideline based on the latest evidence-based pre- and re-habilitation strategies and is designed for seamless integration into routine clinical practice. By facilitating proactive rehabilitation interventions, it aims to improve outcomes in GI cancer patients who are at high risk of postoperative complications, functional decline, and malnutrition.
- 4,833 View
- 140 Download
Review Article
- Liver Cirrhosis and Sarcopenia
-
Hye Yeon Chon, Tae Hee Lee
- Ann Clin Nutr Metab 2022;14(1):2-9. Published online June 1, 2022
- DOI: https://doi.org/10.15747/ACNM.2022.14.1.2
-
Abstract
PDF
- Malnutrition is one of the most common complications in patients with liver cirrhosis. In previous studies, cirrhotic patients with severe malnutrition have been associated with higher morbidity and mortality rates before and after liver transplantation. Frailty and sarcopenia are phenotypes of severe malnutrition that have been associated with complications requiring hospitalization or mortality during the wait for transplantation in patients with cirrhosis. Tools for evaluating frailty include the Activities of Daily Living scale, the Karnofsky Performance Status scale, and the Liver Frailty Index. Diagnosed by using computed tomography, sarcopenia is measured with the skeletal muscle index at L3 and is normalized by height. Nutritional status should be evaluated within the first 24~48 hours of hospitalization in every patient with cirrhosis. Among the various available screening tools, the Royal Free Hospital-Nutritional Prioritizing Tool proposed in the UK is recommended. Nutritional counseling with a multidisciplinary team is recommended to improve long-term survival in patients with cirrhosis. Multidisciplinary nutrition management should include evaluating nutritional status and providing guidance for achieving nutritional goals. Most guidelines suggest a calorie intake of 25~35 kcal/kg/day, and the recommended protein intake is 1.2~1.5 g/kg/day. One beneficial technique for patients is to divide the total recommended intake across four to five daily meals, including a nighttime snack. The principles of nutritional intervention in cirrhotic patients are not different from those in noncirrhotic patients. For improvement of sarcopenia, a strategic approach including physical activity and exercise, hormone replacement therapy, ammonia-lowering agents, and treatment of underlying liver disease is required.
-
Citations
Citations to this article as recorded by
- Liver fibrosis index and mortality in metabolic dysfunction–associated steatotic liver disease: a Korean cohort study
Yesung Lee, Woncheol Lee
Scientific Reports.2025;[Epub] CrossRef
- Liver fibrosis index and mortality in metabolic dysfunction–associated steatotic liver disease: a Korean cohort study
- 13,667 View
- 77 Download
- 1 Crossref
 First
First Prev
Prev

