 E-submission
E-submission
Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 14(2); 2022 > Article
- Original Article Provision of Enteral Nutrition in the Surgical Intensive Care Unit: A Multicenter Prospective Observational Study
-
Chan-Hee Park, M.D.1
 , Hak-Jae Lee, M.D.2, Suk-Kyung Hong, M.D., Ph.D.2, Yang-Hee Jun, M.D., Ph.D.2, Jeong-Woo Lee, M.D.1, Nak-Jun Choi, M.D.3, Kyu-Hyouck Kyoung, M.D., Ph.D.4
, Hak-Jae Lee, M.D.2, Suk-Kyung Hong, M.D., Ph.D.2, Yang-Hee Jun, M.D., Ph.D.2, Jeong-Woo Lee, M.D.1, Nak-Jun Choi, M.D.3, Kyu-Hyouck Kyoung, M.D., Ph.D.4 -
DOI: https://doi.org/10.15747/ACNM.2022.14.2.66
Published online: December 1, 2022
1Division of Trauma Surgery, Department of Surgery, Keimyung University Dongsan Medical Center, Daegu, Korea
2Division of Acute Care Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
3Division of Acute Care Surgery, Department of Surgery, Korea University Guro Hospital, Seoul, Korea
4Department of Trauma Surgery, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea
- Corresponding author: Hak-Jae Lee E-mail lhj206@hanmail.net ORCID https://orcid.org/0000-0002-7016-5076
• Received: October 25, 2022 • Revised: November 12, 2022 • Accepted: November 14, 2022
© The Korean Society of Surgical Metabolism and Nutrition and The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 649 Views
- 13 Download
Abstract
-
Purpose Timely enteral nutrition (EN) is important in critically ill patients. However, use of EN with critically ill surgical patients has many limitations. This study aimed to analyze the current status of EN in surgical intensive care units (ICUs) in South Korea.
-
Materials and Methods A multicenter, prospective, observational study was conducted on patients who received EN in surgical ICUs at four university hospitals between August 2021 and January 2022.
-
Results This study included 125 patients. The mean time to start EN after admission to the surgical ICU was 6.2±4.6 days. EN was provided to 34 (27.2%) patients within 3 days after ICU admission. At 15.7±15.9 days, the target caloric requirement was achieved by 74 (59.2%) patients through EN alone. Furthermore, 104 (83.2%) patients received supplemental parenteral nutrition after a mean of 3.5±2.1 days. Only one of the four hospitals regularly used enteral feeding tubes and post-pyloric feeding tubes.
-
Conclusion Establishing EN guidelines for critically ill surgical patients and setting an appropriate insurance fee for EN-related devices, such as the feeding pump and enteral feeding tube, are necessary.
INTRODUCTION
Appropriate nutritional support is crucial in intensive care of critically ill patients. Adequate nutrition is imperative for critically ill surgical patients who experience many metabolic changes in response to injuries caused by surgery or trauma. Adequate nutritional support helps increase immunity, maintain the intestinal mucosal barrier, and promote wound recovery. However, many difficulties are encountered in providing proper nutrition to critically ill surgical patients [1,2].
The importance of enteral nutrition (EN) in critically ill patients is constantly being emphasized. In fact, the guidelines of the American Society for Parenteral and Enteral Nutrition (ASPEN) and the European Society for Parenteral and Enteral Nutrition (ESPEN) recommend early implementation of EN upon stable status of critically ill patients [3,4]. In these guidelines, early EN is recommended to be performed within 24~48 hours after fluid resuscitation and patient stabilization. However, in actual clinical settings, many difficulties are encountered in early implementation of EN in critically ill patients. In critically ill surgical patients, EN can be hindered by abdominal trauma, changes in anatomy after abdominal surgery, and frequent occurrence of gastrointestinal complications, such as ileus and bleeding.
Given the many difficulties in applying EN at an early period, we need to know what causes EN to be delayed in clinical practice. Currently, studies on the current status of EN in surgical intensive care units (ICUs) in South Korea are unavailable. Therefore, we prospectively analyzed how EN was performed in the surgical ICU of four university hospitals in South Korea.
MATERIALS AND METHODS
This study prospectively investigated the status of EN among patients admitted to the surgical ICU of four university hospitals (Asan Medical Center, Keimyung University Dongsan Medical Center, Korea University Guro Hospital, Ulsan University Hospital) in South Korea from August 2021 to January 2022. We included only patients who stayed in the ICU for more than 48 hours and excluded those with EN limitations due to short bowel syndrome or anastomosis leak.
The Institutional Review Board (IRB) of Asan Medical Center approved this study (IRB no. 2021-0686). Patient data were prospectively collected from electrical medical records for analysis. Informed consent was obtained from all patients or families before collection and analysis of data.
The primary outcomes are time of first EN administration in the ICU and duration to achieve target caloric requirement through EN. The secondary outcomes were types of EN solutions and feeding pumps and number of patients who received supplemental parenteral nutrition (PN). Next, we investigated the reasons for EN discontinuation and measures for EN maladaptation. The causes of EN maladaptation were divided into gastrointestinal problems (excess gastric residual volume [GRV], aspiration, diarrhea, etc.), gastrointestinal bleeding, hemodynamic instability, and repeated procedures or surgery. We also determined use of post-pyloric feeding tube and gastrostomy or jejunostomy.
The target caloric requirement was calculated using the recommendation of the American College of Chest Physicians (ACCP) (25 kcal/kg of usual body weight) [5]. Feeding interruption was defined as fasting for more than 24 hours after EN initiation. Excessive GRV was defined as ≥300 mL drainage through a feeding tube over 6 hours.
We divided reason for ICU admission into three categories: (1) medical problems such as pneumonia or urinary tract infection; (2) surgical problems such as anastomosis leakage, bowel perforation, or postoperative bleeding; and (3) trauma.
We summarized the data as mean and standard deviation for continuous variables and number and percentage for categorical variables. Continuous variables were compared using Student’s t-test and the Mann–Whitney U-test. The Kruskal–Wallis test was used for multiple-group comparisons. Post-hoc analysis was performed using the Bonferroni method. A P-value less than 0.05 was considered statistically significant. All statistical data were analyzed using R software (version 4.0.3; R Foundation for Statistical Computing, Vienna, Austria; http://www.R-project.org).
RESULTS
A total of 978 patients was admitted to the surgical ICU of the four hospitals over the 6-month study period. Of these, 546 were discharged within 2 days for postoperative monitoring. Among those who stayed in the ICU for more than 3 days, 245 did not receive EN for various reasons. Ultimately, 125 patients were included in this study (Fig. 1).
We analyzed the EN-related devices and protocols in the surgical ICU of four hospitals (Table 1). Usually, 16~18 EN solutions were available, 4~10 of which were ready to hang (RTH). Two hospitals (A and C) regularly used a feeding pump for EN. Each hospital had nutritional support team (NST) consultation systems and an EN protocol for each ICU, except for one hospital (D).
We summarized the EN-related characteristics of the study participants (Table 2). The mean length of ICU stay for patients in the ICU for more than 3 days and who received EN was 26.2 days. In addition, the average time to start EN after admission to the ICU was 6.2 days. Thirty-four patients received EN within 3 days, as suggested in the guidelines. The most common reason for not initiating EN within 3 days was unstable vital signs (43.9%), followed by persistent postoperative ileus (26.4%). During the ICU stay, 74 (59.2%) patients achieved the target caloric requirement by EN alone, at a mean of 15.7 days. Supplemental PN was provided to 104 (83.2%) patients and started at a mean of 3.5 days after initiation of EN.
During the ICU period, 66 (52.8%) patients paused EN for various reasons, including excessive GRV and diarrhea. In addition, 10 patients paused EN because of repeated surgeries or procedures. In patients with feeding interruption, interventions such as change of medication dose, treatment with Clostridium difficile, and fasting were applied. Furthermore, 12 (18.2%) patients received a post-pyloric feeding tube.
The status of EN was analyzed by hospital (Table 3). Although the start of EN was delayed to a mean of 7.7 days in one hospital, the mean time of onset among the other hospitals was 4~6 days. Within 3 days, 12.2%~48.0% of the patients started EN. Among all hospitals, more than 60% of the patients received supplemental PN starting at a mean of 2.6 days to 7.0 days after initiation of EN. With the exception of one hospital, enteral feeding tubes and post-pyloric feeding tubes were rarely used. In two hospitals, some patients underwent gastrostomy.
Finally, we compared the timing of EN and PN according to reason for ICU admission (Table 4). Patients with surgical problems started EN at an average of 7.4 days after ICU admission, which was much later than for patients with medical problems or trauma (Fig. 2). However, use of supplemental PN was similar across the groups.
DISCUSSION
Adequate nutritional support in critically ill patients is essential for their recovery. In particular, the importance of EN has been emphasized. Several guidelines have reported that early EN reduces mortality and infectious complications [3,4,6]. However, early EN implementation has many barriers in the actual clinical setting [7,8]. Initiation of EN and achievement of target calories often are delayed in surgical ICU patients compared to nonsurgical ICU patients [1,9,10]. Drover et al. [1] reported the status of nutritional support in 167 surgical ICUs in 21 countries. EN was provided for 54.6% of critically ill surgical patients compared to 77.8% in critically ill medical patients. The average initiation time of EN in surgical ICU patients was 57.8 hours, which was later than the 36.8 hours in medical ICU patients [1]. As such, in South Korea, for better EN support in the surgical ICU, the current status of EN must be determined in this region. Given the lack of studies focusing on this matter, the present study was performed.
This study was conducted in the surgical ICU of four domestic hospitals, and the bed capacity of these participating hospitals ranged from 900 to 2,700 beds. As shown in Fig. 1, of the 432 patients who stayed in the ICU for more than 3 days, excluding postoperative monitoring, 245 (56.7%) never received EN. Thus, EN was not performed in most ICU patients for various reasons, such as early extubation or agitation. Although this study did not include patients who did not receive EN, further research is needed to verify these findings.
Even among the patients who received EN and were included in this study, EN was initiated at a mean of 6.2 days after ICU admission. The percentage of patients who received early EN within 3 days, as suggested in the guideline, was 27.2%, which is quite small. The main reasons for not performing early EN were unstable vital signs and postoperative ileus. Despite dedicated intensivists and an EN protocol at each hospital, early EN was limited in many patients. In particular, patients who were admitted to the ICU due to surgical problems such as postoperative complications started EN later than those admitted to the ICU for other reasons. Therefore, development of guidelines related to the nutrition of critically ill surgical patients is essential.
In addition, although use of supplemental PN differed between hospitals, it was used in 83.2% of the overall EN patients. The average start time of supplemental PN was 3.5 days after EN initiation, considerably earlier than the time from admission to EN. In critically ill surgical patients who often have poor nutritional status before surgery, supplemental PN is applied earlier than in medically ill patients. However, Casaer et al. [11] reported that the group with early PN initiation had higher rates of infectious complications and mortality compared to those with later PN use. Recently, several studies have reported various results regarding supplemental PN at an early stage. The most recently reported study, which was conducted by Gao et al. [12], revealed that early supplemental PN in patients who underwent major abdominal surgery lowered the frequency of nosocomial infection and showed no significant differences in other outcomes, such as noninfectious complications and adverse events. In South Korea, supplemental PN is applied earlier than in other countries; hence, more research is needed on the timing of supplemental PN in critically ill surgical patients.
Although EN was performed in the ICU, more than 50% of the patients had to pause EN because of excessive GRV, diarrhea, aspiration, or repeated surgery or procedure, which limit use of EN in critically ill patients [13,14]. For better course of EN, every hospital should implement an EN protocol [15,16].
In some situations, hospitals in South Korea have problems regarding EN devices. Although the guidelines recommend use of a feeding pump and enteral feeding tube, these devices were used regularly in only one participating hospital. Most hospitals used the Levin tube for EN supply, but this device may cause problems such as gastrointestinal bleeding. Additionally, most of the hospitals were providing continuous EN infusion without an EN-specific feeding pump, leading to problems such as blockages and infusion dose errors. To address such issues, hospitals need to establish an insurance fee for EN-related devices such as a feeding pump and enteral feeding tube.
Insertion of a post-pyloric feeding tube is recommended when the risk of repeat aspiration is high; however, it was performed only in one hospital in the present study [3,4,17]. Post-pyloric feeding tube insertion requires the help of a gastroenterologist or an interventional radiologist, but in reality, there are not many experiences with this procedure in South Korea. Therefore, to improve this problem, the hospital should develop an educational program and make an appropriate insurance fee for this procedure.
This study has several limitations. First, it was conducted as a multicenter study but included only four hospitals, achieving a small sample size. Six university hospitals were initially included. However, two of them were designated as coronavirus disease 2019 (COVID-19)-specific and allowed limited treatment of critically ill surgical patients. Therefore, we excluded these two hospitals. Multicenter studies with more hospitals are needed in future research.
Second, although it was conducted as a prospective study, obtaining informed consent was difficult because visits were restricted during the COVID-19 pandemic. Consequently, all eligible patients could not participate, indicating the possibility of selection bias.
CONCLUSION
In conclusion, early implementation of EN in critically ill surgical patients has many limitations. Accordingly, new EN guidelines that fit the reality of these patients should be established. Additionally, EN-related devices such as a feeding pump and enteral feeding tube often produce difficulties, and an EN-related insurance fee must be established.
AUTHOR CONTRIBUTIONS
Conceptualization: HJL, SKH. Data Curation : HJL, YHJ, JWL, CHP, NJC, KHK. Formal analysis: HJL, YHJ. Funding acquisition: HJL. Investigation: HJL, JWL, CHP, NJC, KHK. Methodology: HJL, SKH. Project administration: HJL, JWL, CHP, NJC, KHK. Resources: HJL, YHJ. Software: HJL. Supervision: SKH, KHK. Validation: HJL, YHJ. Visualization: HJL, CHP. Writing – original draft: CHP. Writing – review & editing: HJL, CHP.
CONFLICTS OF INTEREST
The authors of this manuscript have no conflicts of interest to disclose.
FUNDING
This work was supported by the Korean Society of Surgical Metabolism and Nutrition (KSSMN).
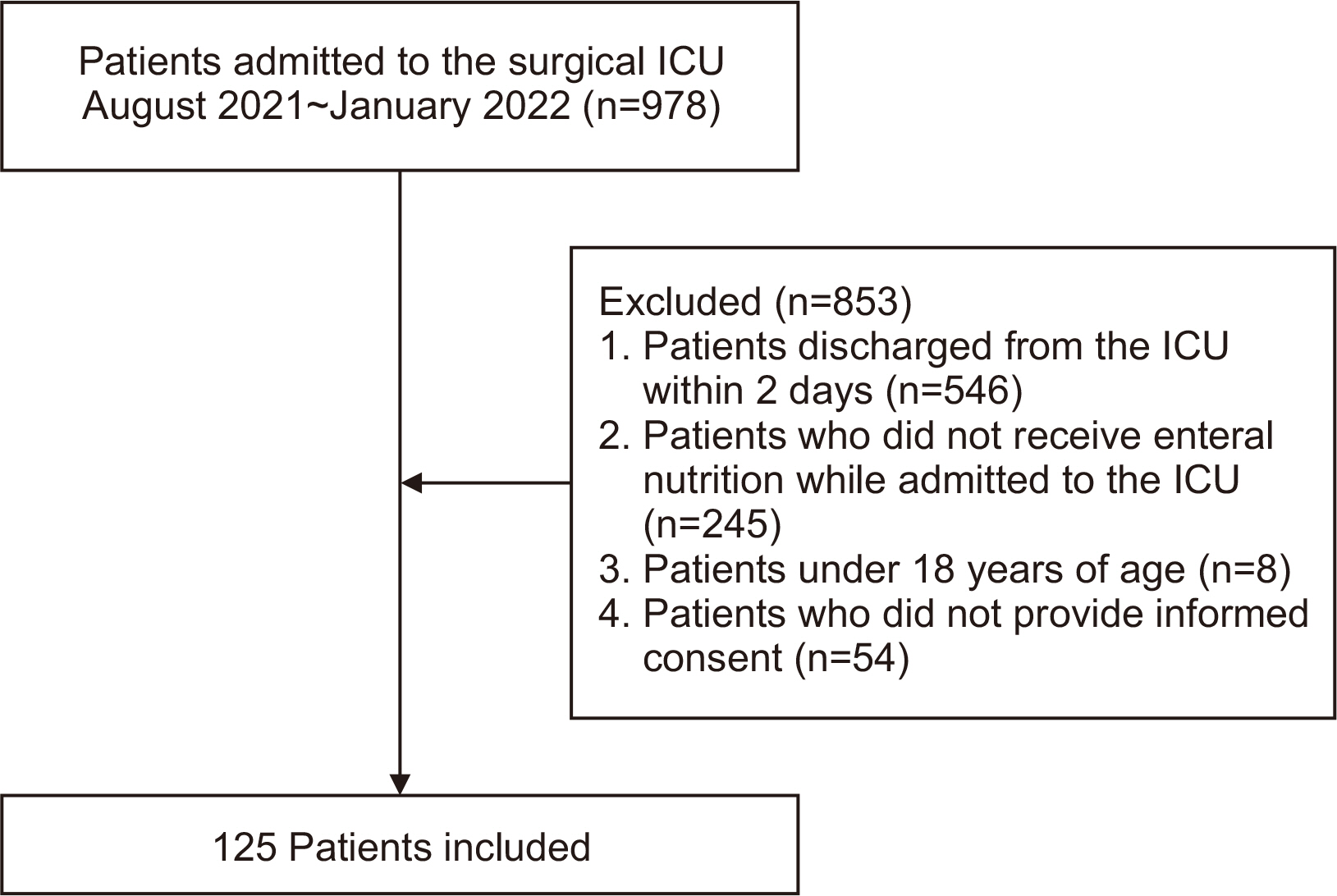
Fig. 2
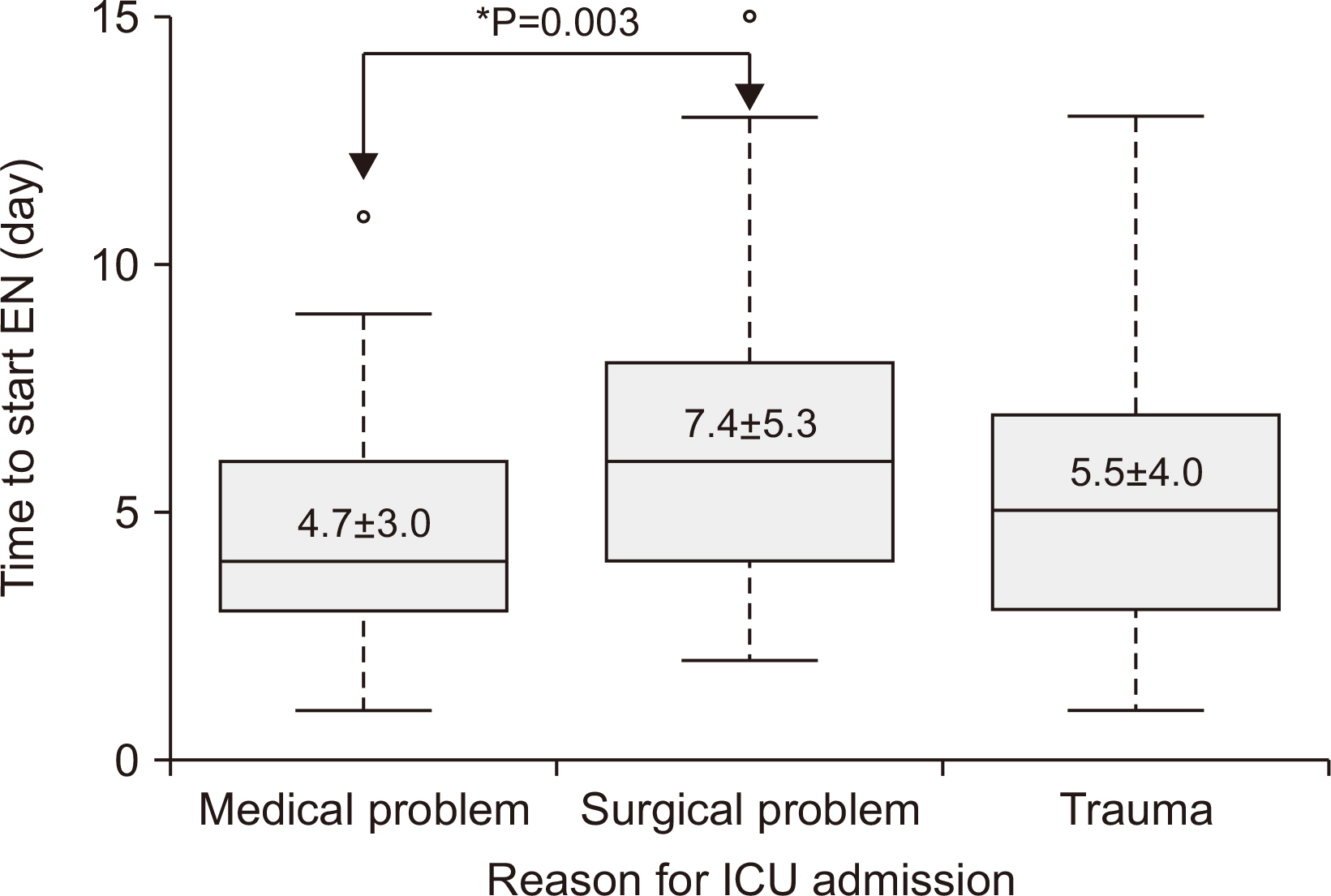
Post-hoc analysis between timing of enteral nutrition (EN) and reason for intensive care unit (ICU) admission.
Table 1
Status of enteral nutrition in the surgical intensive care units of four participating hospitals
Table 2
Clinical characteristics associated with EN
Table 3
Comparison of EN characteristics by hospital
Table 4
EN and PN statistics according to reason for ICU admission
| Characteristics | Medical problem (n=35) | Surgical problem (n=64) | Trauma (n=26) | P-value |
|---|---|---|---|---|
| Time to start EN after ICU admission (day) | 4.7±3.0a | 7.4±5.3a | 5.5±4.0 | 0.012* |
| Patients who received EN within 3 days | 15 (42.9)a | 8 (12.5)a | 11 (42.3) | 0.001* |
| Achievement of target caloric requirement with EN (day) | 12.4±12.6 | 20.2±19.7 | 16.6±15.8 | 0.100 |
| Use of supplemental PN | 29 (82.9) | 53 (82.8) | 22 (84.6) | 0.977 |
| Time to start supplemental PN after instillation of EN (day) | 3.1±1.8 | 3.6±1.6 | 3.8±3.4 | 0.472 |
- 1. Drover JW, Cahill NE, Kutsogiannis J, Pagliarello G, Wischmeyer P, Wang M, et al. Nutrition therapy for the critically ill surgical patient: we need to do better! JPEN J Parenter Enteral Nutr 2010;34:644-52. PubMed
- 2. Kim BC, Lee IK, Kim EY. Analysis of current status and predisposing factors for nutritional support of patients in surgical intensive care unit. Surg Metab Nutr 2016;7:32-8. Article
- 3. McClave SA, Taylor BE, Martindale RG, Warren MM, Johnson DR, Braunschweig C, et al. American Society for Parenteral and Enteral Nutrition. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr 2016;40:159-211; Erratum in: JPEN J Parenter Enteral Nutr 2016;40:1200. PubMed
- 4. Singer P, Blaser AR, Berger MM, Alhazzani W, Calder PC, Casaer MP, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr 2019;38:48-79. ArticlePubMed
- 5. Cerra FB, Benitez MR, Blackburn GL, Irwin RS, Jeejeebhoy K, Katz DP, et al. Applied nutrition in ICU patients. A consensus statement of the American College of Chest Physicians. Chest 1997;111:769-78. ArticlePubMed
- 6. Reintam Blaser A, Starkopf J, Alhazzani W, Berger MM, Casaer MP, Deane AM, et al. ESICM Working Group on Gastrointestinal Function. Early enteral nutrition in critically ill patients: ESICM clinical practice guidelines. Intensive Care Med 2017;43:380-98. ArticlePubMedPMCPDF
- 7. Chang SJ, Kim H. Barriers to enteral feeding of critically ill adults in Korea. Asia Pac J Clin Nutr 2019;28:238-45.PubMed
- 8. Habib M, Murtaza HG, Kharadi N, Mehreen T, Ilyas A, Khan AH, et al. Interruptions to enteral nutrition in critically ill patients in the intensive care unit. Cureus 2022;14:e22821. ArticlePubMedPMC
- 9. Hise ME, Halterman K, Gajewski BJ, Parkhurst M, Moncure M, Brown JC. 2007;Feeding practices of severely ill intensive care unit patients: an evaluation of energy sources and clinical outcomes. J Am Diet Assoc 107:458-65. ArticlePubMed
- 10. Factum CS, de Souza Moreira TH, Rocha CDN, Saldanha MF, Silva FM, Jansen AK. Calorie and protein delivery in critically ill surgical and non-surgical patients receiving enteral nutrition therapy. Rev Chil Nutr 2020;47:916-24. Article
- 11. Casaer MP, Mesotten D, Hermans G, Wouters PJ, Schetz M, Meyfroidt G, et al. Early versus late parenteral nutrition in critically ill adults. N Engl J Med 2011;365:506-17. ArticlePubMed
- 12. Gao X, Liu Y, Zhang L, Zhou D, Tian F, Gao T, et al. Effect of early vs late supplemental parenteral nutrition in patients undergoing abdominal surgery: a randomized clinical trial. JAMA Surg 2022;157:384-93. PubMedPMC
- 13. Seol EM, Kwon KS, Kim JG, Kim JT, Kim J, Moon SM, et al. Nutritional therapy related complications in hospitalized adult patients: a Korean multicenter trial. J Clin Nutr 2019;11:12-22. Article
- 14. Kim H, Stotts NA, Froelicher ES, Engler MM, Porter C. Enteral nutritional intake in adult Korean intensive care patients. Am J Crit Care 2013;22:126-35. ArticlePubMedPMCPDF
- 15. Chinda P, Poomthong P, Toadithep P, Thanakiattiwibun C, Chaiwat O. The implementation of a nutrition protocol in a surgical intensive care unit; a randomized controlled trial at a tertiary care hospital. PLoS One 2020;15:e0231777. ArticlePubMedPMC
- 16. Park H, Lim SY, Kim S, Kim HS, Kim S, Yoon HI, et al. 2022;Effect of a nutritional support protocol on enteral nutrition and clinical outcomes of critically ill patients: a retrospective cohort study. Acute Crit Care 37:382-90. ArticlePubMedPMCPDF
- 17. Preiser JC, Arabi YM, Berger MM, Casaer M, McClave S, Montejo-González JC, et al. A guide to enteral nutrition in intensive care units: 10 expert tips for the daily practice. Crit Care 2021;25:424.ArticlePubMedPMCPDF
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteProvision of Enteral Nutrition in the Surgical Intensive Care Unit: A Multicenter Prospective Observational Study
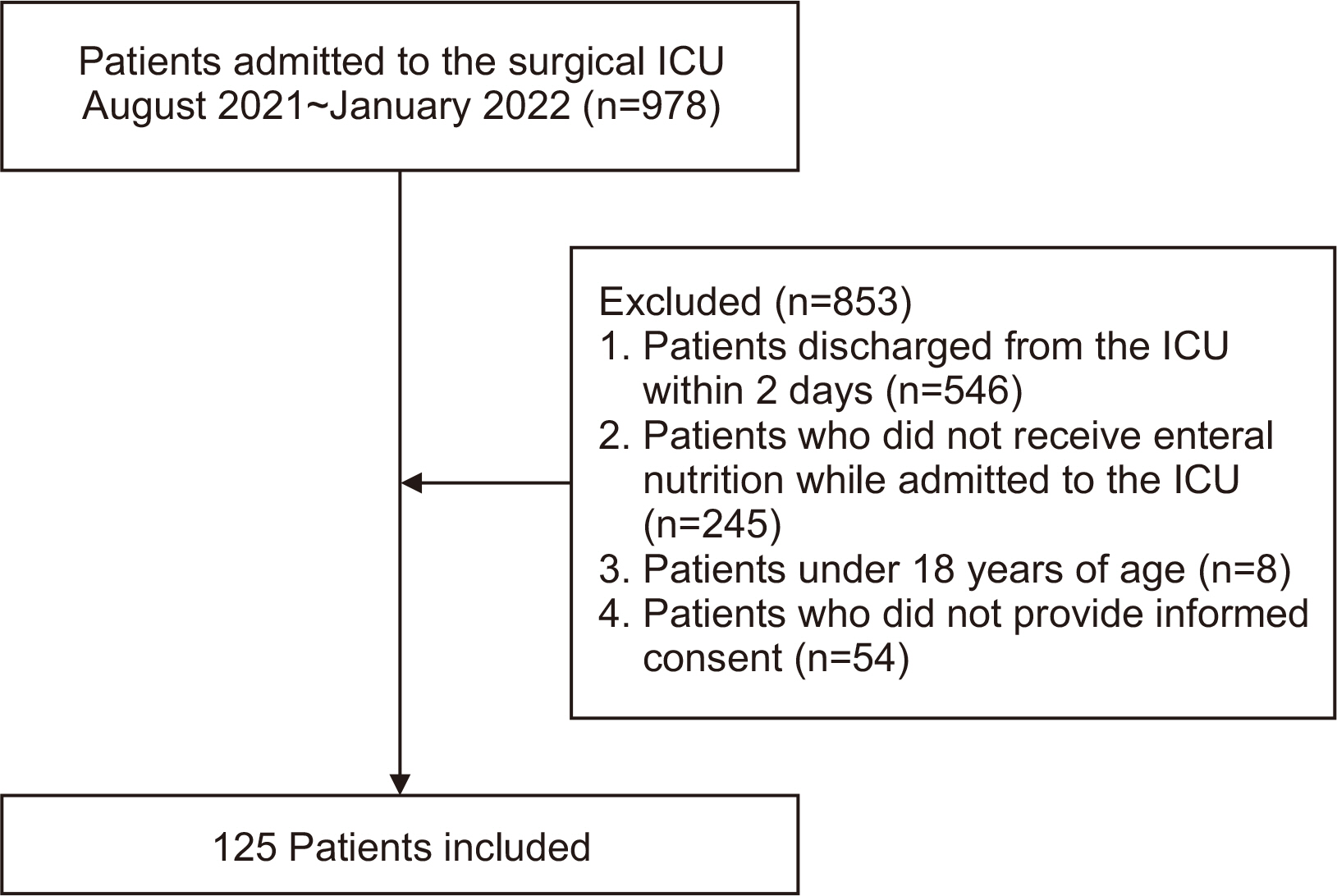
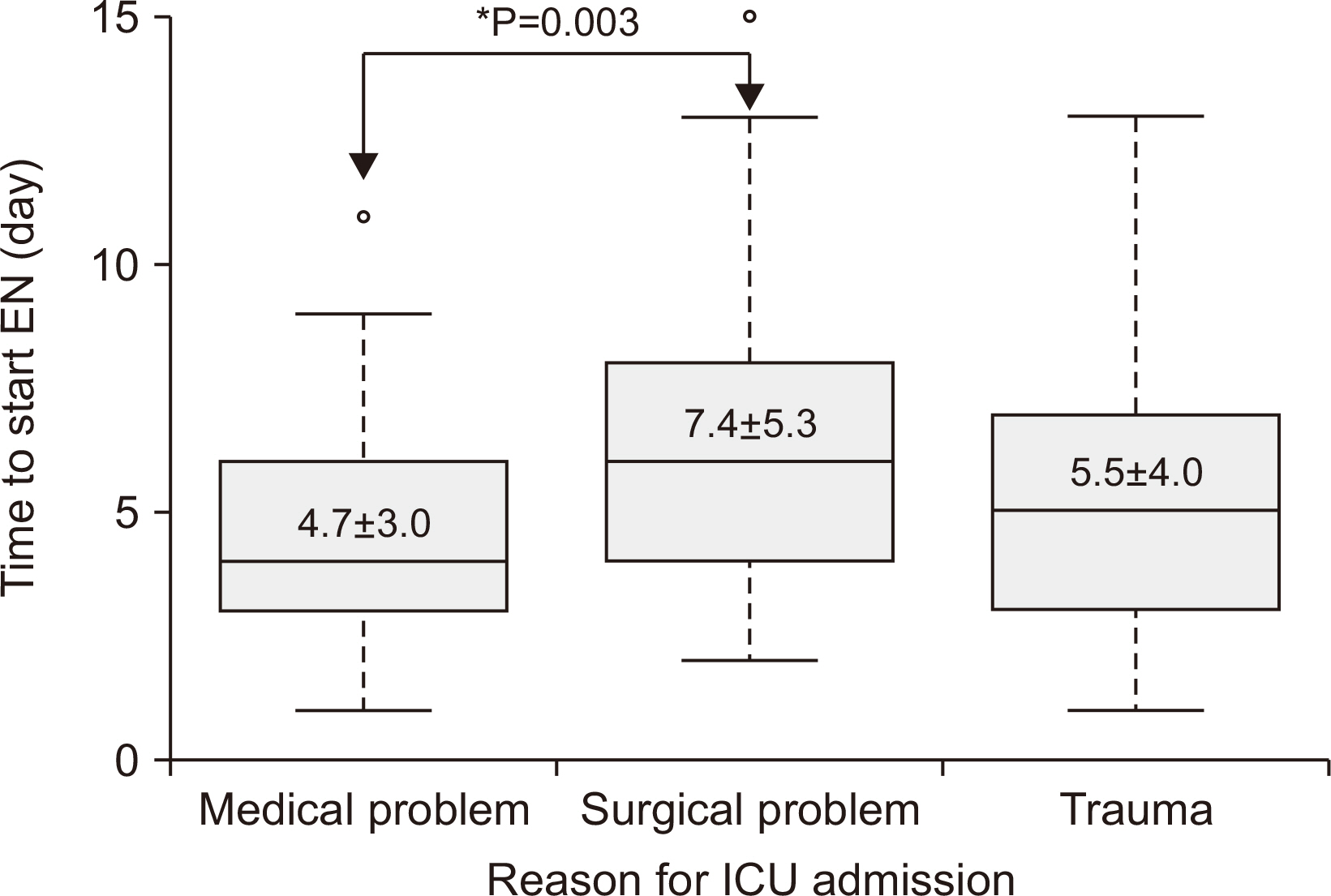
Fig. 1
Patient selection in this study.
ICU = intensive care unit.
Fig. 2
Post-hoc analysis between timing of enteral nutrition (EN) and reason for intensive care unit (ICU) admission.
Fig. 1
Fig. 2
Provision of Enteral Nutrition in the Surgical Intensive Care Unit: A Multicenter Prospective Observational Study
Status of enteral nutrition in the surgical intensive care units of four participating hospitals
| Hospital | Number of surgical ICU beds | Number of EN solutions prescribed in the ICU (RTH, non-RTH) | Regular use of a feeding pump in the ICU | Average number of feeding pumps used per day | NST consult for ICU patients | EN protocol in the ICU |
|---|---|---|---|---|---|---|
| A | 14 | 16 (4, 12) | Yes | 6~10 | Yes | Yes |
| B | 16 | 17 (10, 7) | No | 2~4 | Yes | Yes |
| C | 20 | 16 (7, 9) | Yes | 3 | Yes | Yes |
| D | 14 | 18 (8, 10) | No | 2 | Yes | No |
ICU = intensive care unit; EN = enteral nutrition; RTH = ready to hang; NST = nutritional support team.
Clinical characteristics associated with EN
| Characteristics | Value (n=125) |
|---|---|
| Age (yr) | 65.98±16.97 |
| Sex (male) | 73 (58.4) |
| Reason for ICU admission | |
| Postoperative monitoring | 29 (23.2) |
| Sepsis | 49 (39.2) |
| Trauma | 22 (17.6) |
| Respiratory failure | 12 (9.6) |
| Other | 13 (10.4) |
| Length of ICU stay (day) | 26.2±23.9 |
| Length of hospital stay (day) | 58.65±40.6 |
| Time to EN after ICU admission (day) | 6.2±4.6 |
| Patients who received EN within 3 days | 34 (27.2) |
| Reason for not starting EN within 3 days (among 91 patients) | |
| Unstable vital sign | 40 (44.0) |
| Anastomosis leakage | 24 (26.4) |
| Gastrointestinal bleeding | 4 (4.4) |
| Ileus | 2 (2.2) |
| Other | 21 (23.1) |
| Administration of EN solution at outset | |
| Continuous feeding | 118 (94.4) |
| Intermittent feeding | 7 (5.6) |
| Achievement of target caloric requirement by EN alone | 74 (59.2) |
| Time of achievement of target caloric requirement with EN (day) (among 74 patients) | 15.7±15.9 |
| Use of supplemental PN | 104 (83.2) |
| Time to start supplemental PN after instillation of EN (day) (among 104 patients) | 3.5±2.1 |
| Patients who underwent feeding interruption | 66 (52.8) |
| Reason for feeding interruption (among 66 patients) | |
| Excess GRV | 22 (33.3) |
| Diarrhea | 9 (13.6) |
| Aspiration | 7 (10.6) |
| Gastrointestinal bleeding | 3 (4.5) |
| Unstable vital sign | 5 (7.6) |
| Repeat procedure or operation | 10 (15.2) |
| Other | 10 (15.2) |
| Intervention for feeding interruption (among 66 patients) | |
| Change of medication dose | 30 (45.5) |
| Treatment with Clostridium difficile | 3 (4.5) |
| Insertion of post-pyloric feeding tube | 12 (18.2) |
| No oral food intake (NPO) | 19 (28.8) |
| Other (PTGBD, colostomy) | 2 (3.0) |
Values are presented as mean±standard deviation or number (%).
EN = enteral nutrition; ICU = intensive care unit; PN = parenteral nutrition; GRV = gastric residual volume; NPO = nil per os; PTGBD = percutaneous transhepatic gallbladder drainage.
Comparison of EN characteristics by hospital
| Hospital | Number of enrolled patients | Time to start EN (day) | Patients who received EN within 3 days | Use of supplemental PN | Time to start supplemental PN (day) | Use of enteral feeding tube | Use of post-pyloric feeding tube | Use of gastrostomy |
|---|---|---|---|---|---|---|---|---|
| A | 54 | 5.9±3.6 | 15 (27.8) | 43 (79.6) | 4.1±1.6 | 24 (44.4) | 11 (20.4) | 5 (9.3) |
| B | 25 | 4.7±3.7 | 12 (48.0) | 19 (76.0) | 3.5±3.3 | 0 | 0 | 0 |
| C | 5 | 4.4±1.9 | 2 (40.0) | 3 (60.0) | 7.0±4.6 | 0 | 1 (20.0) | 0 |
| D | 41 | 7.7±6.1 | 5 (12.2) | 39 (95.1) | 2.6±0.8 | 2 (4.9) | 0 | 6 (14.6) |
Values are presented as mean±standard deviation or number (%).
EN = enteral nutrition; PN = parenteral nutrition.
EN and PN statistics according to reason for ICU admission
| Characteristics | Medical problem (n=35) | Surgical problem (n=64) | Trauma (n=26) | P-value |
|---|---|---|---|---|
| Time to start EN after ICU admission (day) | 4.7±3.0 |
7.4±5.3 |
5.5±4.0 | 0.012 |
| Patients who received EN within 3 days | 15 (42.9) |
8 (12.5) |
11 (42.3) | 0.001 |
| Achievement of target caloric requirement with EN (day) | 12.4±12.6 | 20.2±19.7 | 16.6±15.8 | 0.100 |
| Use of supplemental PN | 29 (82.9) | 53 (82.8) | 22 (84.6) | 0.977 |
| Time to start supplemental PN after instillation of EN (day) | 3.1±1.8 | 3.6±1.6 | 3.8±3.4 | 0.472 |
Values are presented as mean±standard deviation or number (%).
EN = enteral nutrition; PN = parenteral nutrition; ICU = intensive care unit.
aPost-hoc analysis was performed by Bonferroni method. *P-value <0.05.
Table 1
Status of enteral nutrition in the surgical intensive care units of four participating hospitals
ICU = intensive care unit; EN = enteral nutrition; RTH = ready to hang; NST = nutritional support team.
Table 2
Clinical characteristics associated with EN
Values are presented as mean±standard deviation or number (%). EN = enteral nutrition; ICU = intensive care unit; PN = parenteral nutrition; GRV = gastric residual volume; NPO = nil per os; PTGBD = percutaneous transhepatic gallbladder drainage.
Table 3
Comparison of EN characteristics by hospital
Values are presented as mean±standard deviation or number (%). EN = enteral nutrition; PN = parenteral nutrition.
Table 4
EN and PN statistics according to reason for ICU admission
Values are presented as mean±standard deviation or number (%). EN = enteral nutrition; PN = parenteral nutrition; ICU = intensive care unit. aPost-hoc analysis was performed by Bonferroni method. *P-value <0.05.

