
Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 16(2); 2024 > Article
- Review Definition, assessments, and current research on sarcopenia in children: a narrative review
-
Min-Jung Bang

-
Annals of Clinical Nutrition and Metabolism 2024;16(2):49-56.
DOI: https://doi.org/10.15747/ACNM.2024.16.2.49
Published online: August 1, 2024
Division of Pediatric Surgery, Department of Surgery, Ajou University School of Medicine, Suwon, Korea
- Corresponding author: Min-Jung Bang, email: ventvertb@gmail.com
• Received: May 23, 2024 • Revised: July 21, 2024 • Accepted: July 26, 2024
© 2024 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 222 Views
- 7 Download
Abstract
-
Purpose Sarcopenia is a well-established prognostic factor for the clinical outcomes of adult patients with cancer and chronic diseases and correlates with increased intensive care unit admissions and prolonged hospital stays. However, research on sarcopenia in children is limited due to its undefined criteria and a lack of studies exploring its impact on clinical outcomes.
-
Current concept The challenges in pediatric sarcopenia research include the absence of standardized body composition methods to quantify muscle mass and muscular function, as well as inconsistencies in definitions. Additionally, there is a lack of age- and gender-specific normative data, particularly for young children and infants. Most studies also lack assessments of muscle function, which can lead to bias and misclassification of sarcopenia. The field is further hindered by poor study quality, limited outcome-focused research, and a dearth of longitudinal data. While some studies suggest that various diseases can affect children’s lean muscle mass, few have linked changes in muscle mass to clinical outcomes.
-
Conclusion The existing literature on pediatric sarcopenia and its relationship with medical and surgical outcomes is sparse and indicates poorer outcomes associated with sarcopenia. Although extensive research has established a link between sarcopenia and adverse outcomes in adults, information on its impact in pediatric populations remains scarce. Further studies are needed to elucidate the association between muscle mass and outcomes in pediatric surgical patients.
Introduction
According to a definition first published by the European Working Group on Sarcopenia in Older People (EWGSOP) in 2010, sarcopenia is a syndrome defined by progressive and generalized loss of skeletal muscle mass (SMM) and strength, which increase the risk of physical impairment, poor quality of life, and mortality [1]. Since muscle strength is currently the most accurate indicator of muscle function, EWGSOP2 employs low muscle strength as the main criterion for sarcopenia in its 2018 definition (Table 1) [2].
There is a general expectation that sarcopenia in pediatric patients may also influence the prognosis of diseases; however, research on sarcopenia in this population is limited compared to that in adults. Moreover, there is a challenge in defining sarcopenia in pediatric patients using the criteria outlined in EWGSOP2 because it is not as simple to apply them as it is in adults.
The purposes of this review were to explore the diagnostic criteria; to assess the knowledge gap in the methodological considerations to define pediatric sarcopenia; and to provide an overview of the existing clinical research that conducted to assess illnesses which that negatively affect muscle metabolism in the pediatric population and the clinical outcomes of medical and surgical pediatric patients with sarcopenia.
Definition and pathophysiology of sarcopenia
Primary sarcopenia occurs through a combination of generalized muscle fiber loss, a decrease in fast units, neurodegeneration, and aging-related protein metabolic changes [1]. When there is a demonstrable contributing factor to sarcopenia other than age, it is classified as secondary [2]. Secondary sarcopenia in adults can be caused by insulin resistance; physical inactivity; malnutrition; neuromuscular illnesses; and an imbalance in sex hormones, growth hormones, thyroid hormones, glucocorticoids, or vitamin D metabolism (Fig. 1) [3]. Systemic inflammatory processes, as seen in end organ failure, chronic inflammatory diseases, endocrine disorders, and cancer, also lead to a progressive and widespread reduction in SMM. In these circumstances, cytokine-mediated inflammation promotes a catabolic state, which mobilizes and degrades proteins and muscle mass [4].
Owing to the scarcity of epidemiological evidence and standardized diagnostic criteria concerning sarcopenia among children, assessing its prevalence in the pediatric population remains difficult. However, the following have been proposed as potential causes of sarcopenia in pediatric populations: metabolic syndrome, physical inactivity, nutritional deficiencies, perinatal and genetic factors, vitamin D deficiency, endocrinopathy, dysbiosis of the gut microbiota, neuromuscular diseases, organ failure, malignant tumors, and other inflammatory disorders (Fig. 2) [5,6].
The diagnostic criteria for adult sarcopenia are well described by the EWGSOP2, which suggests assessment of sarcopenia using grip strength or chair stand measures with specific cut-off points of <27 kg for men, <16 kg for women, and >15 seconds for five rises. Confirming sarcopenia requires the detection of low muscle quantity and quality. In clinical settings, dual-energy X-ray absorptiometry (DXA) is typically used to measure the appendicular skeletal muscle mass (ASM). In research studies, the ASM or SMM is often measured using DXA, bioelectrical impedance analysis (BIA), computed tomography (CT), or magnetic resonance imaging. The cut-off points for ASM are <20 kg for men and <16 kg for women. The value of ASM/height2 is also used with cut-off points of <7.0 kg/m2 for men and <5.5 kg/m2 for women. A severity assessment can be conducted through performance measures such as gait speed (cut-off value≤0.8 m/s), short physical performance battery (cut-off value≤8 point score), timed up and go test (cut-off value≥20 seconds), and the 400-meter walk test (positive=non-completion or ≥6 min for completion) [2].
A significant barrier in investigating sarcopenia in children is the absence of a consensus regarding its definition and diagnostic criteria [7]. This absence is partially explained by a lack of age-specific and gender-specific normative data for muscle mass, particularly in the pediatric group. However, employing the adult diagnostic criteria to pediatric patients presents practical challenges, and distinct criteria are required from those used for adults. Consequently, previous studies utilized various methodologies to define pediatric sarcopenia. However, none integrated muscle function assessment, which potentially leads to bias and misclassification of sarcopenia. Every investigation included an assessment of muscle mass, but most did not provide a mechanism for distinguishing abnormal from normal muscle mass.
One study diagnosed sarcopenia in novel ways either by defining it as a SMM z-score<–2 (as measured by DXA) [8] or as less than average measurements of both SMM and handgrip strength. In contrast, another research group utilized psoas muscle volume and patient stature to devise a sarcopenia index and defined sarcopenia as a reduction in the sarcopenia index relative to healthy counterparts [9]. Lurz et al. [10] employed the psoas muscle area (PMA) index (PMA/height2) as an indicator of sarcopenia, assessing tPMA (total PMA) at L3–L4 and L4–L5 via computed tomography imaging in pediatric patients with end-stage liver disease (ESLD). Another group of researchers applied a change in psoas muscle volume to define sarcopenia [11]. One research cohort quantified psoas muscle volume and subsequently constructed a receiver operating characteristic curve that delineated sarcopenia as a percentage decline in muscle mass greater than 1.0 [12]. Suzuki et al. [13] formulated a muscle loss index by standardizing the discrepancy in psoas muscle volume pre- and post-treatment and designated the sarcopenic cohort as those falling within the lowest quartile. The diversity in defining sarcopenia across studies underscores a notable gap in research and warrants further exploration. According to recent research trends, PMA measurements from cross-sectional abdominal CT images are an easily accessible and reproducible method of assessing the presence of sarcopenia [14]. PMA measurements extracted from CT scans have been employed in research endeavors examining pediatric sarcopenia within diverse patient populations, including those with leukemia, ESLD, chronic renal disease, and intestinal failure [9,10,13,15]. One beneficial tool for evaluating pediatric sarcopenia is the age- and gender-specific reference values for tPMA in children, which are available through online platforms (https://ahrc-apps.shinyapps.io/sarcopenia/) [16]. Notably, tPMA z-scores have been employed in four recent studies to evaluate sarcopenia, alongside the analysis of clinical outcomes in pediatric malignant and chronic disorders. Although the tPMA z-score has been widely used in recent studies, more well-designed research is necessary to evaluate its potential as a noble diagnostic criterion for pediatric sarcopenia.
The heterogeneity in the definition of pediatric sarcopenia, coupled with the absence of standardized methodologies to measure muscle mass or conduct muscular function assessments, presents challenges in accurately evaluating the condition. Moreover, there is a notable dearth of age- and gender-specific normative data for muscle mass, particularly in infants and young children. Furthermore, the omission of muscular function evaluation in current investigations could introduce bias and result in misclassification of sarcopenia.
Although there are no clear integrated diagnostic criteria for pediatric sarcopenia, some studies revealed that pediatric patients suffer “sarcopenia” in relation to various illnesses. Mangus et al. [9] reported significant sarcopenia among pediatric patients with end-stage liver, kidney, and intestinal failure by scaling the PMA on CT images in relation to patient height. Similarly, Lurz et al. [10] found that children diagnosed with ESLD prior to liver transplantation (LT) exhibited reduced tPMA (measured at L3–L4 and L4–L5 on CT imaging) compared to that of healthy controls matched for age and gender. Furthermore, a decrease in muscle mass has been described in children shortly after diagnosis with Crohn’s disease and vitamin D deficiency, as well as in children with inflammatory bowel disease [17-19]. Hemophilia and Crohn’s disease both negatively affect muscle mass, highlighting the importance of monitoring and addressing muscle health in these chronic diseases [20].
In pediatric oncology, sarcopenia and muscle mass have been extensively studied in acute lymphoblastic leukemia (ALL). Rayar et al. [21] observed that children diagnosed with ALL manifest a decrease in SMM as detected on DXA scans during the initial stages of treatment. They further noted that the extent of this reduction correlates with the severity of the illness.
Many pediatric patients also experience muscle loss during treatment of their illness. Suzuki et al. [13] conducted measurements of the PMA before and after induction therapy in children with ALL. Their findings revealed that all patients experienced muscle loss during treatment. Moreover, they noted a higher incidence of adverse events during treatment among sarcopenic patients than among those without sarcopenia. In the long term, survivors of ALL are susceptible to sarcopenic obesity, which has detrimental effects on their health-related quality of life [21]. Muscle loss during ALL treatment is significant and persistent, indicating the need for strategies to mitigate muscle wasting during therapy [22].
There is another study that showed a linkage between treatment and pediatric sarcopenia. The use of steroids in biliary atresia impacts growth parameters negatively, potentially leading to decreased overall development in length, weight, and head circumference [23]. According to the research listed above, there is a vicious cycle in which illness and treatment play major roles in causing sarcopenia, which causes various adverse events during treatment.
Pediatric sarcopenia and surgery
According to previous research, sarcopenia before surgery was associated with adverse clinical outcomes in pediatric patients after surgery. Sarcopenia and diminished muscle indicators in children undergoing LT have been linked to heightened risks of surgical complications, prolonged hospital and pediatric intensive care unit stays, elevated rates of re-operation, and augmented mortality risk [8,24,25]. In their retrospective study, Mager et al. [8] determined that persistent sarcopenia after LT (on DXA scans) in children with ESLD is linked to poorer growth and recurrent hospital admissions. Oh et al. [26] demonstrated that low preoperative muscle mass in pediatric patients is a significant predictor of adverse early-postoperative outcomes following the Fontan operation. Takeda et al. [25] found that sarcopenia in infants with biliary atresia undergoing LT is associated with longer operation times, greater blood loss, and higher rates of portal vein stenosis and bloodstream infections than those of infants without sarcopenia; sarcopenia may also predict postoperative outcomes. Ritz et al. [15] reported that sarcopenia was an additional risk factor for relapse in children with high-risk hepatoblastoma. While significant results were not observed, sarcopenia appears to impact graft survival, rate of metastasis, and surgical complications in patients with intestinal transplants, hepatoblastoma, and tetralogy of Fallot, respectively [27-29].
Another study found that surgery causes sarcopenia. López et al. [30] reported that pediatric patients with complicated appendicitis tend to undergo sarcopenic changes characterized by reduction in BMI and PMA during their hospital stay. The mean percentage change in PMA per day during treatment for appendicitis was a decrease of 0.81%. These findings suggest not only that perioperative sarcopenia affects the surgical outcomes, but also that the surgical procedure itself also negatively affects children’s muscle metabolism.
Despite its clinical significance, research on pediatric surgical patients with sarcopenia is in its infancy. While studies examining the association between surgical outcomes and sarcopenia are limited, there has been a recent surge in interest, particularly with the widespread adoption of tPMA z-score-based criteria for pediatric sarcopenia. As a result, research on sarcopenia as a prognostic factor in surgical settings is expanding. According to the findings of Dedhia et al. [17], there is a correlation between reduction in psoas muscle volume and elevated risk of postoperative complications in adolescents with ulcerative colitis undergoing a colectomy. The postoperative complications included infection, wound dehiscence, postoperative leak, intra-abdominal abscess, prolonged ileus, pulmonary embolism, venous thromboembolism, and readmission. However, there were no significant associations found between BMI, preoperative steroids, immunosuppression agent use, and postoperative complication risk. Other studies that used the tPMA z-score as a diagnostic tool are listed in Table 2.
Reduced lean muscle mass in adolescents is a significant risk factor for metabolic syndrome, which underscores the importance of muscle health to prevent cardiovascular complications [31,32]. There have been limited investigations on the relationship between sarcopenia and outcomes in pediatric patients (Table 2). These findings emphasize the critical role of muscle mass in the overall health and recovery of pediatric patients across various conditions and treatments. Regular monitoring and proactive management of muscle health are essential in improving outcomes and quality of life for such patients.
Conclusion
Since sarcopenia was recognized as a major prognostic factor in adults with malignant tumors or chronic illnesses, there have been numerous efforts to investigate similar effects in pediatric patients. However, unlike adults, pediatric patients undergo muscle mass increases due to growth, which makes it challenging to clearly define sarcopenia. Consequently, various attempts have been made to define sarcopenia by measuring muscle mass at different body sites. There is also a growing body of research investigating whether sarcopenia can serve as a predictor of surgical outcomes in pediatric patients. Meaningful results are expected, and future research should focus on clinically feasible diagnostic criteria for sarcopenia, the most suitable imaging modality for screening, and the association between sarcopenia and outcomes in pediatric illnesses.
Supplementary materials
None.
Acknowledgments
None.
Conflict of interest
The author of this manuscript has no conflicts of interest to disclose.
Funding
None.
Data availability
None.
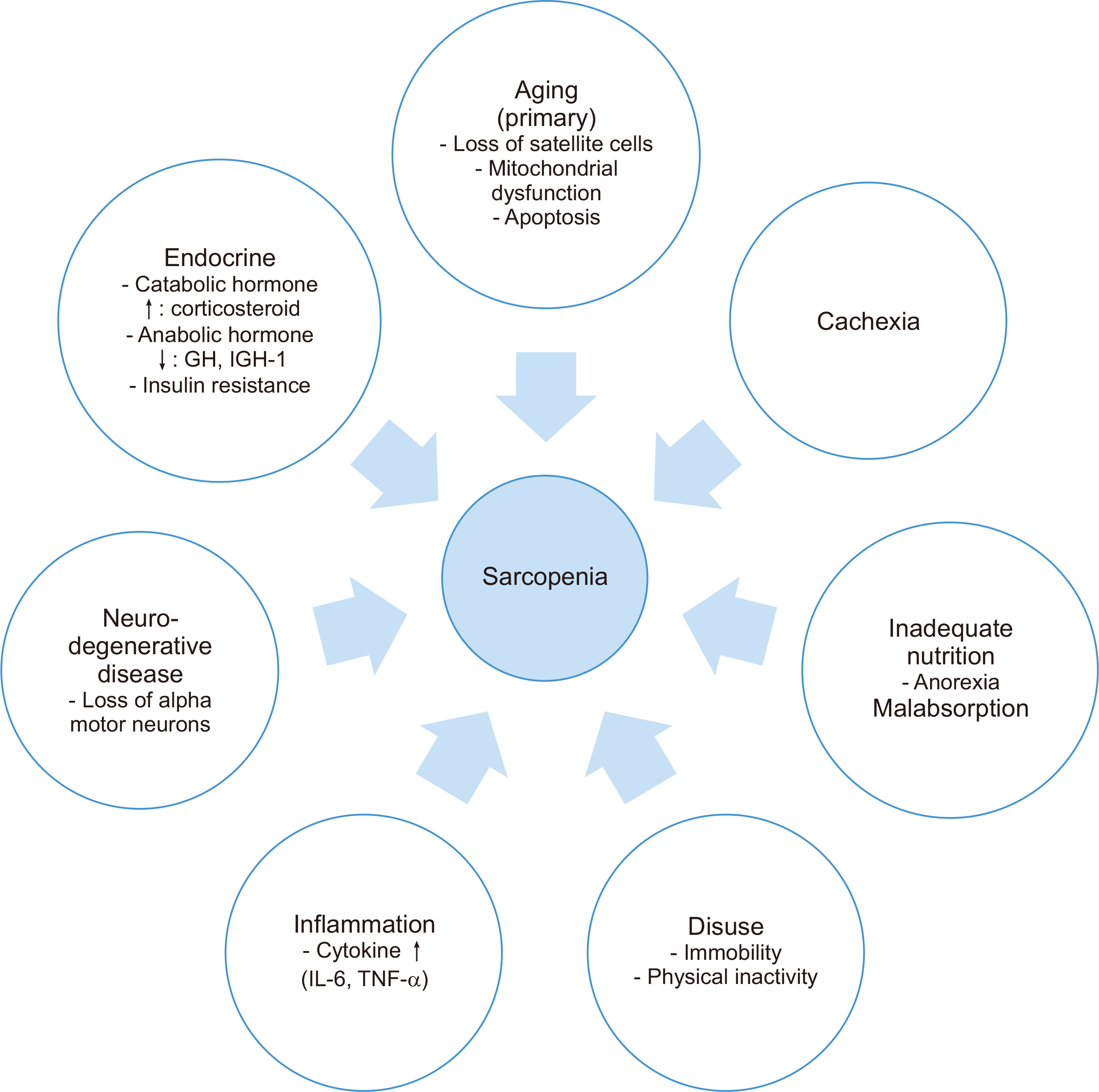
Fig. 2
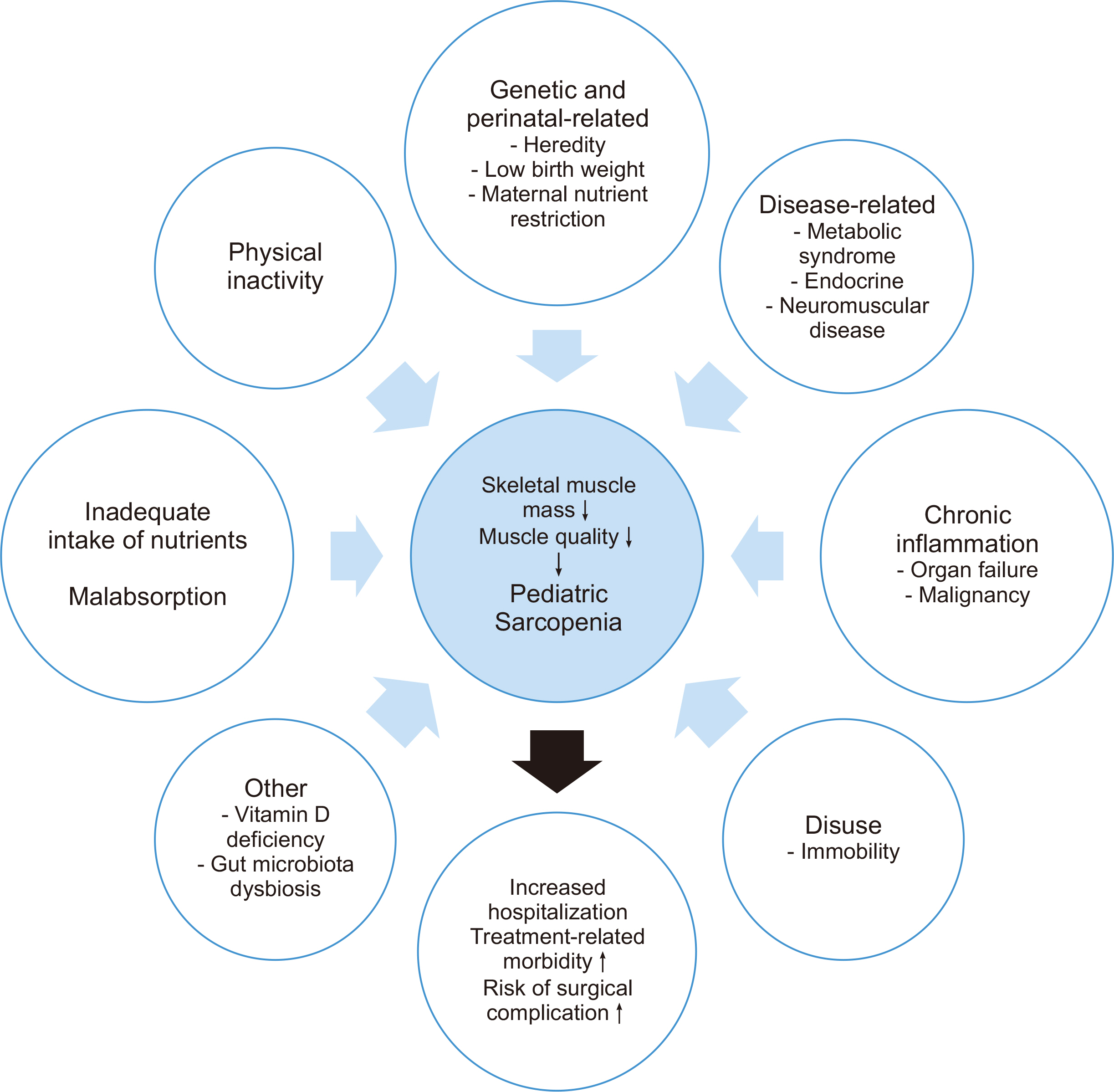
Etiologies of sarcopenia influencing clinical outcomes in children. ↑ = increase; ↓ = decrease.
Table 1
The 2018 operational definition of sarcopenia (EWGSOP2)
Table 2
Summary of current research on pediatric surgical patients with sarcopenia
| Reference | Population | Study design | Sample size (n) | Age (yr) | Methodology or modality | Indicators of muscle mass | Indicators of muscle strength or function | Definition of sarcopenia | Clinical outcome |
|---|---|---|---|---|---|---|---|---|---|
| Dedhia et al., 2018 [17] | Pediatric patients with UC undergoing colectomy | Retrospective | 29 | Range: 13–18 |
MRI L3 |
PSMA and PMA | None | Lowest tertile of PSMA | 62% of patients with post colectomy complications with ulcerative colitis have significantly reduced PSMA |
| López et al., 2017 [30] | Pediatric patients with perforated appendicitis | Retrospective | 36 | Median: 11 |
CT (pre and post op), L3 |
PMA | None | Mean percentage change in PMA index (PMA/height2) |
N/A (Pediatric patients with complex appendicitis experience sarcopenic changes during hospital admission) |
| Mager et al., 2018 [19] | Pediatric post-LT patients | Retrospective | 41 | Range: 0.5–17 | DXA | SMM-z | None | SMM-z <–2SD of age and gender normative values | Sarcopenia was significantly associated with increased hospitalization and ventilator dependency |
| Oh et al., 2019 [26] | Pediatric patients undergoing the Fontan operation | Retrospective | 74 | Range: 2.8–3.3 |
CT (pre and post op) |
Bilateral pectoralis muscles (T2) and erector spinae muscles (T12) | None | None | Preoperative low muscle mass was associated with poor early postoperative outcomes in pediatric patients undergoing the Fontan operation |
| Takeda et al., 2021 [25] | Children with LTfor biliary atresia | Retrospective | 89 | Range: 0.6–0.7 |
CT (pre and post op) L3 and L4 |
PMA | None | tPMA-z<–2 | Sarcopenia in infants with BA may be associated with patient survival and serve as an effective marker for post-operative outcomes of LT |
| Ritz et al., 2021 [15] | Children with hepato-blastoma | Retrospective | 33 | Range: 1.2–3.0 |
CT and MRI L3–L4 and L4–L5 |
PMA | None | tPMA-z<–2 | Sarcopenia was an additional risk factor for relapse in children with high-risk HB |
| Raghu et al., 2022 [27] | Pediatric intestinal transplant recipient | Retrospective | 56 | Range: 1.8–9.8 |
CT L3–L4 and L4–L5 |
PMA | None | tPMA-z<–2 |
N/A (Sarcopenia was not associated with decreased graft survival) |
| Muñoz-Serrano et al., 2023 [28] | Children with hepato-blastoma | Retrospective | 21 | Median: 3 | MRI | PMA | None | tPMA-z<–2 |
N/A (Sarcopenia at diagnosis was associated with higher rates of metastases and surgical complications) |
| Jang et al., 2023 [29] | Pediatric patients undergoing total correction of TOF | Retrospective | 330 | Mean: 5 | Chest CT(pre and post op) | Bilateral pectoralis muscles (T2) and erector spinae muscles (T12) | None | MMI-z<–2 |
N/A (Preoperative sarcopenia did not predict early postoperative major adverse events) |
UC = ulcerative colitis; LT = liver transplantation; TOF = tetralogy of Fallot; MRI = magnetic resonance imaging; CT = computed tomography; op = operative; DXA = dual-energy X-ray absorptiometry; PSMA = paraspinous muscle area; PMA = psoas muscle area; SMM-z = skeletal muscle mass z-score; SD = standard deviation; tPMA-z = total psoas muscle area z-score; N/A = not assessed; BA = biliary atresia; HB = hepatoblastoma.
- 1. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010;39:412-23. PubMedPMC
- 2. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019;48:16-31. ArticlePubMedPDF
- 3. Thomas DR. Loss of skeletal muscle mass in aging: examining the relationship of starvation, sarcopenia and cachexia. Clin Nutr 2007;26:389-99. ArticlePubMed
- 4. Triarico S, Rinninella E, Mele MC, Cintoni M, Attinà G, Ruggiero A. Prognostic impact of sarcopenia in children with cancer: a focus on the psoas muscle area (PMA) imaging in the clinical practice. Eur J Clin Nutr 2022;76:783-8. ArticlePubMedPDF
- 5. Jung HN, Jung CH, Hwang YC. Sarcopenia in youth. Metabolism 2023;144:155557. ArticlePubMed
- 6. Mager DR, Hager A, Gilmour S. 2023;Challenges and physiological implications of sarcopenia in children and youth in health and disease. Curr Opin Clin Nutr Metab Care 26:528-33. ArticlePubMed
- 7. Ooi PH, Thompson-Hodgetts S, Pritchard-Wiart L, Gilmour SM, Mager DR. Pediatric sarcopenia: a paradigm in the overall definition of malnutrition in children? JPEN J Parenter Enteral Nutr 2020;44:407-18. ArticlePubMedPDF
- 8. Mager DR, Hager A, Ooi PH, Siminoski K, Gilmour SM, Yap JYK. Persistence of sarcopenia after pediatric liver transplantation is associated with poorer growth and recurrent hospital admissions. JPEN J Parenter Enteral Nutr 2019;43:271-80. ArticlePubMedPDF
- 9. Mangus RS, Bush WJ, Miller C, Kubal CA. Severe sarcopenia and increased fat stores in pediatric patients with liver, kidney, or intestine failure. J Pediatr Gastroenterol Nutr 2017;65:579-83. ArticlePubMed
- 10. Lurz E, Patel H, Frimpong RG, Ricciuto A, Kehar M, Wales PW, et al. Sarcopenia in children with end-stage liver disease. J Pediatr Gastroenterol Nutr 2018;66:222-6. ArticlePubMed
- 11. Rezende IFB, Conceição-Machado MEP, Souza VS, Santos EMD, Silva LR. Sarcopenia in children and adolescents with chronic liver disease. J Pediatr (Rio J) 2020;96:439-46. ArticlePubMed
- 12. Kawakubo N, Kinoshita Y, Souzaki R, Koga Y, Oba U, Ohga S, et al. The Influence of sarcopenia on high-risk neuroblastoma. J Surg Res 2019;236:101-5. ArticlePubMed
- 13. Suzuki D, Kobayashi R, Sano H, Hori D, Kobayashi K. Sarcopenia after induction therapy in childhood acute lymphoblastic leukemia: its clinical significance. Int J Hematol 2018;107:486-9. ArticlePubMedPDF
- 14. Amini B, Boyle SP, Boutin RD, Lenchik L. Approaches to assessment of muscle mass and myosteatosis on computed tomography: a systematic review. J Gerontol A Biol Sci Med Sci 2019;74:1671-8. ArticlePubMedPMCPDF
- 15. Ritz A, Kolorz J, Hubertus J, Ley-Zaporozhan J, von Schweinitz D, Koletzko S, et al. Sarcopenia is a prognostic outcome marker in children with high-risk hepatoblastoma. Pediatr Blood Cancer 2021;68:e28862. ArticlePubMedPDF
- 16. Lurz E, Patel H, Lebovic G, Quammie C, Woolfson JP, Perez M, et al. 2020;Paediatric reference values for total psoas muscle area. J Cachexia Sarcopenia Muscle 11:405-14. ArticlePubMedPMCPDF
- 17. Dedhia PH, White Y, Dillman JR, Adler J, Jarboe MD, Teitelbaum DH, et al. Reduced paraspinous muscle area is associated with post-colectomy complications in children with ulcerative colitis. J Pediatr Surg 2018;53:477-82. ArticlePubMed
- 18. Atlan L, Cohen S, Shiran S, Sira LB, Pratt LT, Yerushalmy-Feler A. Sarcopenia is a predictor for adverse clinical outcome in pediatric inflammatory bowel disease. J Pediatr Gastroenterol Nutr 2021;72:883-8. ArticlePubMed
- 19. Mager DR, Carroll MW, Wine E, Siminoski K, MacDonald K, Kluthe CL, et al. Vitamin D status and risk for sarcopenia in youth with inflammatory bowel diseases. Eur J Clin Nutr 2018;72:623-6. ArticlePubMedPDF
- 20. Davies A, Nixon A, Muhammed R, Tsintzas K, Kirkham S, Stephens FB, et al. Reduced skeletal muscle protein balance in paediatric Crohn's disease. Clin Nutr 2020;39:1250-7. ArticlePubMed
- 21. Rayar M, Webber CE, Nayiager T, Sala A, Barr RD. Sarcopenia in children with acute lymphoblastic leukemia. J Pediatr Hematol Oncol 2013;35:98-102. ArticlePubMed
- 22. Mueske NM, Mittelman SD, Wren TAL, Gilsanz V, Orgel E. Myosteatosis in adolescents and young adults treated for acute lymphoblastic leukemia. Leuk Lymphoma 2019;60:3146-53. ArticlePubMedPMC
- 23. Alonso EM, Ye W, Hawthorne K, Venkat V, Loomes KM, Mack CL, et al. Impact of steroid therapy on early growth in infants with biliary atresia: the multicenter steroids in biliary atresia randomized trial. J Pediatr 2018;202:179-85.e4. ArticlePubMedPMC
- 24. Woolfson JP, Perez M, Chavhan GB, Johara FT, Lurz E, Kamath BM, et al. Sarcopenia in children with end-stage liver disease on the transplant waiting list. Liver Transpl 2021;27:641-51. ArticlePubMedPMCPDF
- 25. Takeda M, Sakamoto S, Uchida H, Shimizu S, Yanagi Y, Fukuda A, et al. Impact of sarcopenia in infants with liver transplantation for biliary atresia. Pediatr Transplant 2021;25:e13950. ArticlePubMedPDF
- 26. Oh J, Shin WJ, Jeong D, Yun TJ, Park CS, Choi ES, et al. 2019;Low muscle mass as a prognostic factor for early postoperative outcomes in pediatric patients undergoing the fontan operation: a retrospective cohort study. J Clin Med 8:1257.ArticlePubMedPMC
- 27. Raghu VK, Sico R, Rudolph JA, Mazariegos GV, Squires J, Squires JE. Sarcopenia prevalence in pediatric intestinal transplant recipients: Implications on post-transplant outcomes. Pediatr Transplant 2022;26:e14256. ArticlePubMedPDF
- 28. Muñoz-Serrano AJ, Estefanía-Fernández K, Oterino C, Ramírez-Amoros C, Navarro G, Sastre A, et al. 2023;Sarcopenia as a prognostic factor in patients with hepatoblastoma: does it influence surgical outcomes and survival? Preliminary retrospective study. J Pediatr Surg 58:2149-55. ArticlePubMed
- 29. Jang HY, Shin WJ, Jeong D, Baek J, Song IK. Association between preoperative sarcopenia and early postoperative outcomes in pediatric patients undergoing total correction of tetralogy of fallot: a retrospective cohort study. J Cardiothorac Vasc Anesth 2023;37:2020-6. ArticlePubMed
- 30. López JJ, Cooper JN, Albert B, Adler B, King D, Minneci PC. Sarcopenia in children with perforated appendicitis. J Surg Res 2017;220:1-5. ArticlePubMed
- 31. Burrows R, Correa-Burrows P, Reyes M, Blanco E, Albala C, Gahagan S. Low muscle mass is associated with cardiometabolic risk regardless of nutritional status in adolescents: a cross-sectional study in a chilean birth cohort. Pediatr Diabetes 2017;18:895-902. ArticlePubMedPMCPDF
- 32. Kim JH, Park YS. Low muscle mass is associated with metabolic syndrome in Korean adolescents: the Korea National Health and Nutrition Examination Survey 2009-2011. Nutr Res 2016;36:1423-8. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CiteDefinition, assessments, and current research on sarcopenia in children: a narrative review
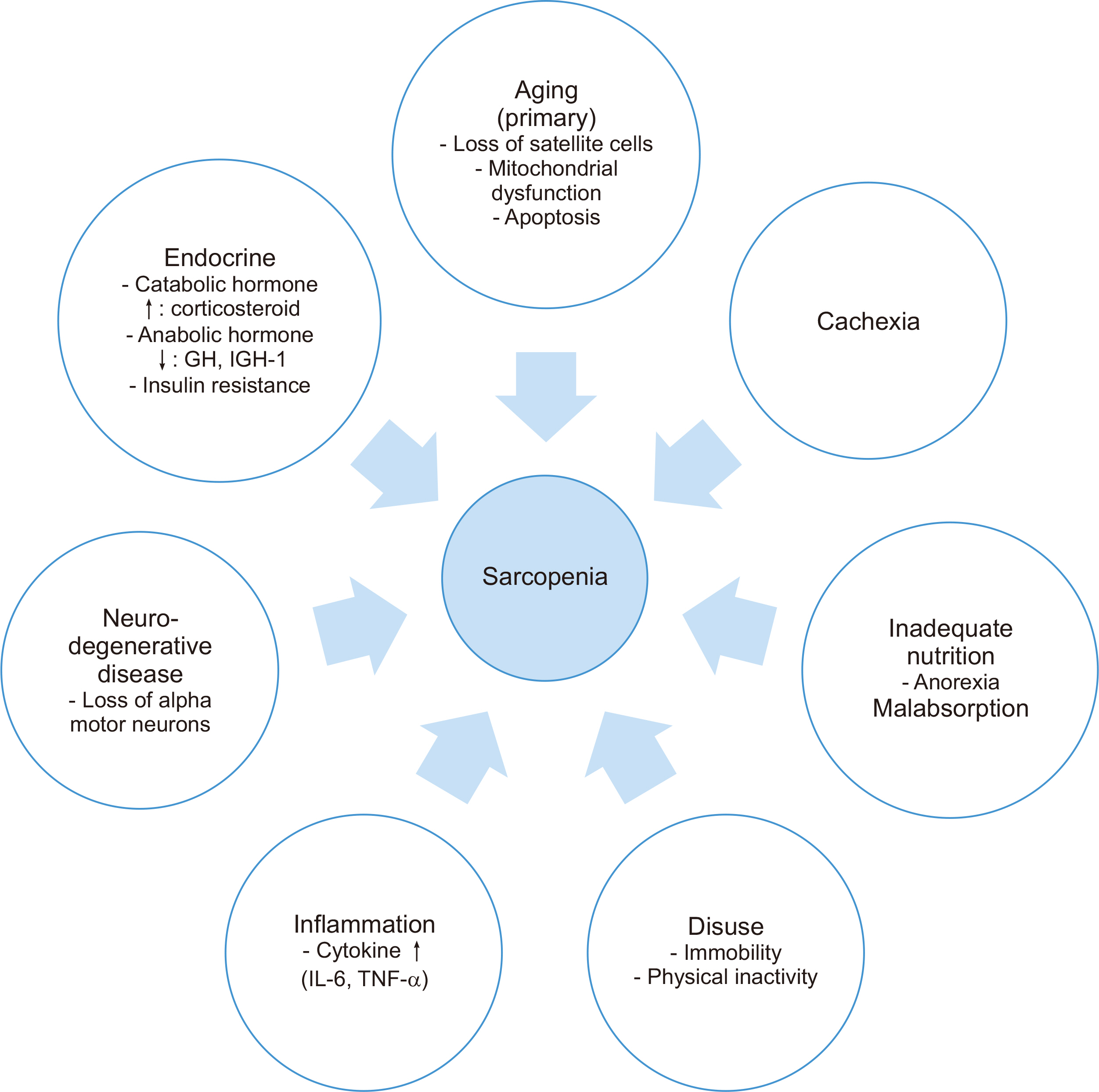
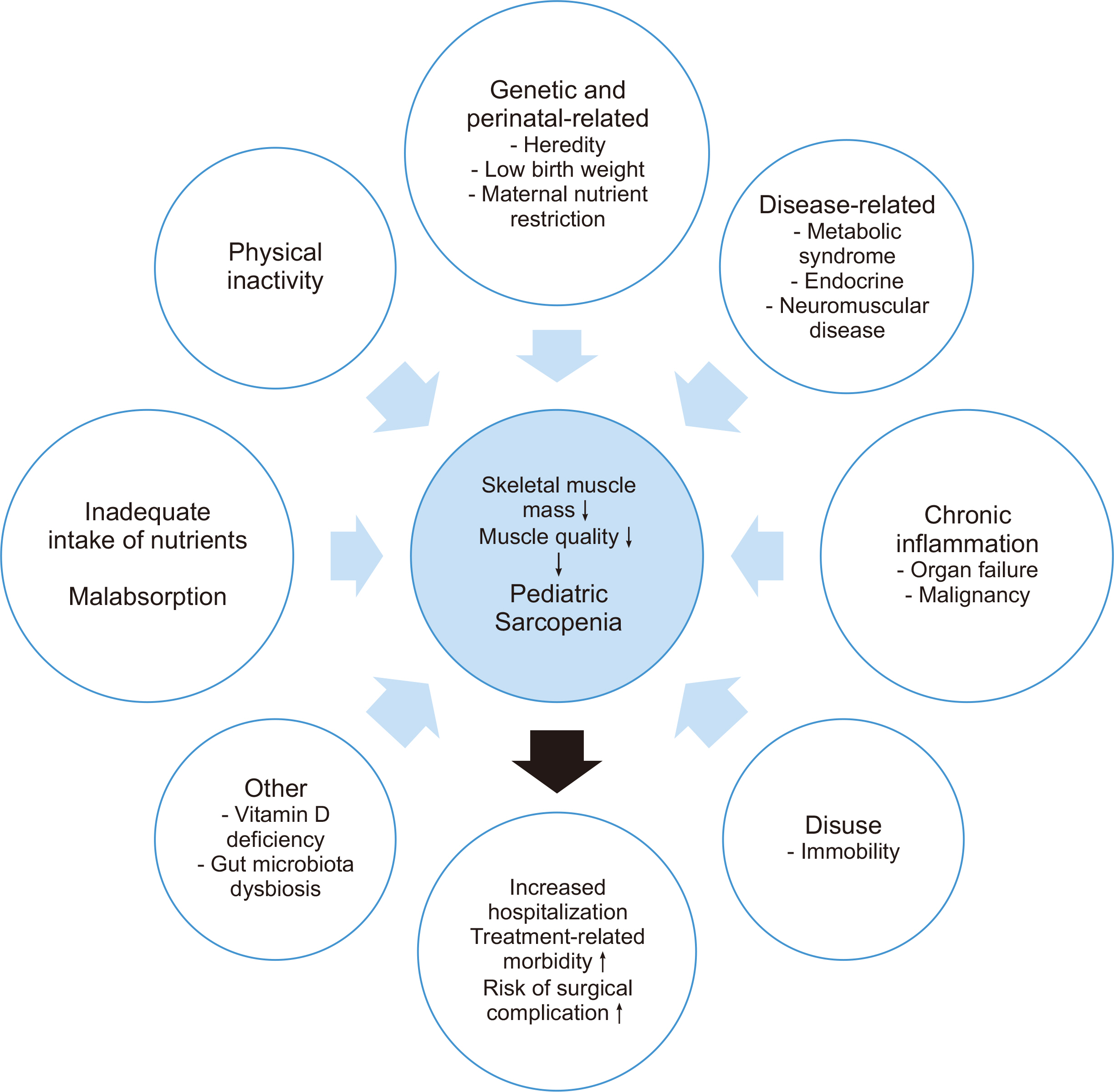
Fig. 1
Mechanisms of sarcopenia in adults. ↑ = increase; ↓ = decrease.
Fig. 2
Etiologies of sarcopenia influencing clinical outcomes in children. ↑ = increase; ↓ = decrease.
Fig. 1
Fig. 2
Definition, assessments, and current research on sarcopenia in children: a narrative review
The 2018 operational definition of sarcopenia (EWGSOP2)
| Criteria | Diagnosis |
|---|---|
| (1) Low muscle strength | Probable sarcopenia is identified by Criterion (1) |
| (2) Low muscle quantity or quality | Diagnosis is confirmed by additional documentation of Criterion (2) |
| (3) Low physical performance | If Criteria (1), (2) and (3) are all met, sarcopenia is considered severe |
Summary of current research on pediatric surgical patients with sarcopenia
| Reference | Population | Study design | Sample size (n) | Age (yr) | Methodology or modality | Indicators of muscle mass | Indicators of muscle strength or function | Definition of sarcopenia | Clinical outcome |
|---|---|---|---|---|---|---|---|---|---|
| Dedhia et al., 2018 [ |
Pediatric patients with UC undergoing colectomy | Retrospective | 29 | Range: 13–18 | MRI L3 |
PSMA and PMA | None | Lowest tertile of PSMA | 62% of patients with post colectomy complications with ulcerative colitis have significantly reduced PSMA |
| López et al., 2017 [ |
Pediatric patients with perforated appendicitis | Retrospective | 36 | Median: 11 | CT (pre and post op), L3 |
PMA | None | Mean percentage change in PMA index (PMA/height2) | N/A (Pediatric patients with complex appendicitis experience sarcopenic changes during hospital admission) |
| Mager et al., 2018 [ |
Pediatric post-LT patients | Retrospective | 41 | Range: 0.5–17 | DXA | SMM-z | None | SMM-z <–2SD of age and gender normative values | Sarcopenia was significantly associated with increased hospitalization and ventilator dependency |
| Oh et al., 2019 [ |
Pediatric patients undergoing the Fontan operation | Retrospective | 74 | Range: 2.8–3.3 | CT (pre and post op) |
Bilateral pectoralis muscles (T2) and erector spinae muscles (T12) | None | None | Preoperative low muscle mass was associated with poor early postoperative outcomes in pediatric patients undergoing the Fontan operation |
| Takeda et al., 2021 [ |
Children with LTfor biliary atresia | Retrospective | 89 | Range: 0.6–0.7 | CT (pre and post op) L3 and L4 |
PMA | None | tPMA-z<–2 | Sarcopenia in infants with BA may be associated with patient survival and serve as an effective marker for post-operative outcomes of LT |
| Ritz et al., 2021 [ |
Children with hepato-blastoma | Retrospective | 33 | Range: 1.2–3.0 | CT and MRI L3–L4 and L4–L5 |
PMA | None | tPMA-z<–2 | Sarcopenia was an additional risk factor for relapse in children with high-risk HB |
| Raghu et al., 2022 [ |
Pediatric intestinal transplant recipient | Retrospective | 56 | Range: 1.8–9.8 | CT L3–L4 and L4–L5 |
PMA | None | tPMA-z<–2 | N/A (Sarcopenia was not associated with decreased graft survival) |
| Muñoz-Serrano et al., 2023 [ |
Children with hepato-blastoma | Retrospective | 21 | Median: 3 | MRI | PMA | None | tPMA-z<–2 | N/A (Sarcopenia at diagnosis was associated with higher rates of metastases and surgical complications) |
| Jang et al., 2023 [ |
Pediatric patients undergoing total correction of TOF | Retrospective | 330 | Mean: 5 | Chest CT(pre and post op) | Bilateral pectoralis muscles (T2) and erector spinae muscles (T12) | None | MMI-z<–2 | N/A (Preoperative sarcopenia did not predict early postoperative major adverse events) |
UC = ulcerative colitis; LT = liver transplantation; TOF = tetralogy of Fallot; MRI = magnetic resonance imaging; CT = computed tomography; op = operative; DXA = dual-energy X-ray absorptiometry; PSMA = paraspinous muscle area; PMA = psoas muscle area; SMM-z = skeletal muscle mass z-score; SD = standard deviation; tPMA-z = total psoas muscle area z-score; N/A = not assessed; BA = biliary atresia; HB = hepatoblastoma.
Table 1
The 2018 operational definition of sarcopenia (EWGSOP2)
Table 2
Summary of current research on pediatric surgical patients with sarcopenia
UC = ulcerative colitis; LT = liver transplantation; TOF = tetralogy of Fallot; MRI = magnetic resonance imaging; CT = computed tomography; op = operative; DXA = dual-energy X-ray absorptiometry; PSMA = paraspinous muscle area; PMA = psoas muscle area; SMM-z = skeletal muscle mass z-score; SD = standard deviation; tPMA-z = total psoas muscle area z-score; N/A = not assessed; BA = biliary atresia; HB = hepatoblastoma.

