 E-submission
E-submission
Articles
- Page Path
- HOME > Ann Clin Nutr Metab > Volume 16(2); 2024 > Article
- Original Article Prognostic significance of serum creatinine and sarcopenia for 5-year overall survival in patients with colorectal cancer in Korea: a comparative study
-
Jiahn Choi1
 , Hye Sun Lee2, Jeonghyun Kang3
, Hye Sun Lee2, Jeonghyun Kang3 -
Annals of Clinical Nutrition and Metabolism 2024;16(2):66-77.
DOI: https://doi.org/10.15747/ACNM.2024.16.2.66
Published online: August 1, 2024
1Yonsei University College of Medicine, Seoul, Korea
2Biostatistics Collaboration Unit, Yonsei University College of Medicine, Seoul, Korea
3Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea
- Corresponding author: Jeonghyun Kang, email: ravic@naver.com
Medical student.
• Received: March 29, 2024 • Revised: May 7, 2024 • Accepted: May 17, 2024
© 2024 The Korean Society of Surgical Metabolism and Nutrition · The Korean Society for Parenteral and Enteral Nutrition
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 643 Views
- 13 Download
Abstract
-
Purpose Previous studies have demonstrated that the serum creatinine level and skeletal muscle index (SMI) (correlated with the overall survival [OS] of patients with colorectal cancer [CRC]). However, the combined significance of these 2 factors is not fully understood. The goal of this study was to investigate the prognostic potential of the combination of these two factors in patients with CRC.
-
Methods The patients were categorized into subgroups based on preoperative serum creatinine level, with a cut-off value of 1.01 mg/dL for males and 0.80 mg/dL for females. The patients were further categorized into 4 groups based on SMI. Data were analyzed using the Cox proportional hazards model and Harrell’s concordance index (C-index).
-
Results Poor 5-year OS was observed in patients with high SMI and high serum creatinine levels (hazard ratio [HR]=1.676, 95% confidence interval [CI]=1.110–2.529, P=0.013), low SMI and low serum creatinine levels (HR=1.916, 95% CI=1.249–2.938, P=0.002), and low SMI and high serum creatinine levels (HR=2.172, 95% CI=1.279–3.687, P=0.004) compared to those of patients with high SMI and low serum creatinine levels. Grouping patients based on both SMI and serum creatinine levels led to improved prognostic stratification (C-index, 0.626; 95% CI=0.587–0.666) compared to grouping based on SMI (CI difference=0.062, 95% CI=0.031–0.103, P=0.0011) or serum creatinine (CI difference=0.043, 95% CI=0.017–0.081, P=0.0072) alone.
-
Conclusion Incorporating both SMI and serum creatinine levels enhances the prognostic stratification for 5-year OS in patients with CRC, surpassing the prognostic power of grouping solely based on SMI or creatinine.
Introduction
Colorectal cancer (CRC) is a common malignant tumor of the gastrointestinal tract, ranking as the third most frequently diagnosed cancer and the second leading cause of cancer-related mortality [1]. Consistent with worldwide epidemiology, in Korea, CRC held the fourth and third positions in terms of the number of new cancer diagnoses among males and females, respectively, in 2020. In that year, it was the third leading cause of cancer-related mortality in males and the second leading cause in females [2].
Sarcopenia, defined as the progressive loss of skeletal muscle mass and function, has emerged as a potential prognostic predictor in patients with cancer [3,4]. Several studies have investigated the association between sarcopenia and overall survival (OS) in various cancer populations and have yielded significant results. A meta-analysis conducted using data from 4,262 patients with ovarian cancer revealed a significant association between skeletal muscle index (SMI) and OS (hazard ratio [HR]=1.11, 95% confidence interval [CI]=1.03–1.20, P=0.007) [3]. Similarly, another meta-analysis on 783 patients with esophageal cancer demonstrated that patients with sarcopenia had decreased OS compared to that of patients without sarcopenia (HR=1.51, 95% CI=1.21–1.89, P=0.0003) [5]. In patients with CRC, sarcopenia was a predictor of overall death (HR=1.28, 95% CI=1.10–1.53) and CRC-related death (HR=1.42, 95% CI=1.13–1.78) compared to patients without sarcopenia [4].
Creatinine, produced in muscles during contraction or metabolism, is closely related to skeletal muscle because it is generated during the breakdown of creatine phosphate [6]. Serum creatinine level has been investigated as a prognostic or predictive marker for CRC. A retrospective cohort study involving 1,254 patients with locally advanced rectal cancer undergoing neoadjuvant chemoradiation before curative-intent surgery reported that patients with chronic kidney disease, defined as estimated creatinine clearance <60 mL/min, had decreased disease-free survival (HR=1.37, 95% CI=1.03–1.82, P=0.03) [7]. Another study including 263 patients with CRC reported that serum creatinine levels were significantly higher in patients with low estimated glomerular filtration rate (eGFR). The overall postoperative complication rate (P=0.048), frequency of severe complications (10% vs. 1%, P<0.01), and length of stay (12.0±10.8 days vs. 9.7±4.5 days, P<0.01) were higher in a lower eGFR group compared to a normal eGFR group [8]. One retrospective study of 3,281 patients with CRC demonstrated that patients with low (HR=2.061, 95% CI=1.454–2.922, P=0.001) or high (HR=1.730, 95% CI=1.423–2.104, P=0.001) creatinine level showed poor 5-year OS compared with patients with normal creatinine level [9].
Considering that creatinine level is closely related to muscle mass, a question arises regarding the relationship between creatinine level and skeletal muscle status, such as in sarcopenia. In one study, combined creatinine and albumin levels were introduced as stratifying factors for sarcopenia, and the 5-year OS rate of the sarcopenia group (conventional patients with sarcopenia with low creatinine×albumin) was only 28.9% compared with 58.9% of non-sarcopenic group (P=0.0005) in 135 patients with esophageal cancer [10]. The results of a previous study suggested a potential relationship between sarcopenia and serum creatinine level in individuals with esophageal cancer. However, few studies have evaluated this correlation in patients with CRC.
We aimed to investigate the potential significance of sarcopenia status and serum creatinine level as prognostic factors in patients with CRC. By assessing these variables, we also aimed to gain insights into their potential role as predictors of patient outcomes, ultimately contributing to personalized treatment strategies and improved survival rates for patients with CRC.
Methods
This study was approved by the Gangnam Severance Hospital Institutional Review Board (3-2023-0001). The requirement for informed consent was waived due to the retrospective nature of the study.
It is a retrospective natured, comparative study of the given patients in grouping. It was described according to the STROBE statement (https://www.strobe-statement.org/).
This study was conducted from July 2006 to February 2014 at Gangnam Severance Hospital, Yonsei University College of Medicine. All patient treated for CRC were targeted. Selected patients were grouped by SMI and serum creatinine level.
The patients were categorized into four groups based on serum creatinine concentration and SMI. Patients who did not have sarcopenia according to the SMI level and with low serum creatinine level were allocated to G1, whereas patients who did not have sarcopenia according to the SMI level with high serum creatinine levels were allocated to G2. Patients who had sarcopenia at the SMI level with low serum creatinine level were allocated to G3, whereas patients who had sarcopenia in the SMI level with high serum creatinine level were allocated to G4.
A total of 1,054 patients with CRC was included in this retrospective study.
Patients who underwent curative resection and were diagnosed as stage I–III CRC, those who underwent abdominopelvic computed tomography (CT), and those who had serum creatinine level measured within 2 months prior to surgery were initially selected.
Patients who met the following conditions were excluded: (1) cell types for CRC of signet ring cell, gastrointestinal stromal tumor, or unknown; (2) tumor location in the appendix, anus, or unknown; (3) CRC of stage 0, stage 4, or no data; (4) undergoing emergency surgery; (5) CRC associated with ulcerative colitis or Crohn’s disease; (6) double primary cancer; (7) inadequate data on SMI and skeletal muscle radiodensity (SMD) measurement, (8) CT not conducted within 2 months prior to surgery, and (9) preoperative creatinine level unavailable. Detailed inclusion criteria are illustrated in Fig. 1.
The primary outcome variables was overall survival, which was defined as the duration from the date of surgery to the date of last follow or death from any cause. Patients with OS periods longer than 5 years were censored. Specifically, the 5-year OS rate from the date of surgery was analyzed in this article. Measured variables were body mass index (BMI) as a SMI and serum creatinine level.
Defining sarcopenia status according to SMI
CT images of the third lumbar spine were selected for measurement of SMI. L3 skeletal muscles, the psoas muscle, the lumbar muscle, the transversus abdominis muscle, the erector spinae, the rectus abdominis, and the internal and external oblique muscles were measured. SMI was calculated by dividing the L3 skeletal muscle cross-sectional area (cm2) by the square of the height (m2). Based on the cut-off value of SMI reported by Martin et al. [11], patients were categorized into sarcopenia and non-sarcopenia groups. Patients with lower SMI (<43 cm2/m2 in males with BMI<25 kg/m2, <53 cm2/m2 in males with BMI≥25 kg/m2, <41 cm2/m2 in females) were assigned to the sarcopenia group, and patients with higher SMI (≥43 cm2/m2 in males with BMI<25 kg/m2, ≥53 cm2/m2 in males with BMI≥25 kg/m2, ≥41 cm2/m2 in females) were assigned to the non-sarcopenia group.
Defining cut-off value of creatinine level according to sex in the X-tile program
The X-tile program was used to define the optimal cut-off value [12]. Based on serum creatinine concentration, patients were categorized into a low creatinine group (<1.01 mg/dL in males and <0.80 mg/dL in females) and high creatinine group (≥1.01 mg/dL in males and ≥0.80 mg/dL in females) (Supplement 1).
There was no selection bias reportable.
Since all target patients were included, no sample size estimation was done.
Within each sex group, a restricted cubic spline (RCS) curve was used to examine the association between serum creatinine level and SMI before surgery and the HR of OS in patients with CRC.
Baseline characteristics were analyzed using chi-square tests or Fisher’s exact test as appropriate for categorical variables
Univariate and multivariable analyses for 5-year OS were conducted using the Cox proportional hazards model; HRs and their corresponding 95% CIs were calculated. Variables identified as significant factors (P<0.05) in the univariate analyses were selected and entered into a multivariable analysis using backward elimination. The Kaplan-Meier method was used to assess the effects of each subgroup on 5-year OS, and the log-rank test was used to compare survival between two or more groups. Additionally, the Harrell’s concordance index (C-index) was used to evaluate the performance of our prognostic model in predicting 5-year OS. The C-index ranges from 0 to 1, with a value of 0.5 implying no discriminatory ability, a value of 1 indicating perfect discrimination, and a higher C-index indicating better prediction performance. A C-index comparison was conducted to evaluate the prognostic model with the best predictive accuracy. Multiple comparisons were conducted by applying the Benjamini-Hochberg procedure.
A P-value<0.05 was considered statistically significant. All analyses were performed using R version 4.2.1 (R-project, Institute for Statistics and Mathematics).
Results
This study included 1,054 patients with CRC and baseline characteristics according to SMI and serum creatinine level as summarized in Table 1. The low-SMI group had a higher proportion of females than the high-SMI group (54.8% vs. 36.2%, P<0.001). The mean BMI of the low SMI group was lower than that of the high SMI group (21.8 kg/m2 vs. 24.1 kg/m2, P<0.001). The mean serum creatinine level of the low SMI group was less than that of the high SMI group (0.8 mg/dL vs. 0.9 mg/dL, P<0.001). No significant differences were observed between the low SMI group and the high SMI group in terms of age, diabetes mellitus (DM), hypertension, smoking, carcinoembryonic antigen (CEA) level, tumor location, histologic grade, lymphovascular invasion (LVI), number of lymph nodes, stage, complications, chemotherapy, or index year.
When patients were categorized into two groups based on serum creatinine levels, the proportion of patients age>70 years was higher in the low creatinine group than in the high creatinine group (73.0% vs. 54.6%, P<0.001). Patients in the high creatinine group were more prone to DM (16.8% vs. 25.2%, P=0.003) and hypertension (37.3% vs. 55.9%, P<0.001). Furthermore, the low creatinine group exhibited a higher percentage of patients with >12 lymph nodes than that of the high creatinine group (88.0% vs. 75.8%, P<0.001). A greater proportion of patients in the high creatinine group experienced complications than that in the low creatinine group (20.1% vs. 29.4%, P=0.001). Patients in the high creatinine group had an earlier index year than patients in the low creatinine group (33.4% vs. 62.7%, P<0.001). No significant differences were observed between the low and high creatinine groups in terms of sex, smoking, BMI, CEA level, tumor location, histologic grade, LVI, stage, chemotherapy, SMI, and SMD (Table 1).
The correlation between SMI and serum creatinine level within each sex group was analyzed using Spearman’s rank correlation test. SMI did not demonstrate a correlation with creatinine level in males (r=0.008, P=0.83) but demonstrated a positive correlation in females (r=0.12, P=0.014; Fig. 2).
The association between serum creatinine level and HR of OS adjusted for sex in patients with CRC is presented using the RCS curve model. A positive correlation was observed in males and females and the HR of OS increased as the preoperative serum creatinine increased in both the low and high serum creatinine groups. With respect to SMI, a negative correlation was observed (Fig. 3).
The Kaplan-Meier curves demonstrated significant differences in OS rates between the non-sarcopenia and sarcopenia groups (P<0.001; Fig. 4A) and between patients with high and low serum creatinine level (P<0.001; Fig. 4B). Differences in 5-year OS rates are depicted in Kaplan-Meier a curve among G1, G2, G3, and G4 in the combined groups (G1-90.8%, G2-79.0%, G3-81.2%, and G4-70.0%), (G1 vs. G2 P<0.001, G1 vs. G3 P<0.001, G1 vs. G4 P<0.001, G2 vs. G3 P=0.658, G2 vs. G4, P=0.129, G3 vs. G4 P=0.091; Fig. 4C).
Similar results were obtained with additional analyses based on sex. In both males and females, patients categorized in the four combined groups exhibited a significant difference in OS according to the Kaplan-Meier survival curve. Among males, the 5-year OS rates were 89.2%, 78.7%, 76.9%, and 70.6% in G1, G2, G3, and G4, respectively, whereas those rates among females were 93.9%, 79.5%, 84.5%, and 69.4%. Moreover, a significant difference was observed in the OS rates of patients in G1 from those of patients in G2, G3, or G4 in both males (G1 vs. G2 P=0.003, G1 vs. G3 P=0.003, G1 vs. G4 P=0.003, G2 vs. G3 P=0.673, G2 vs. G4 P=0.380, G3 vs. G4 P=0.525) and females (G1 vs. G2 P<0.001, G1 vs. G3 P=0.014, G1 vs. G4 P<0.001, G2 vs. G3 P=0.406, G2 vs. G4 P=0.301, G3 vs. G4 P=0.092; Fig. 5).
Univariate analysis was performed to identify the factors affecting OS (Table 2). Age, BMI, CEA, histologic grade, complications, lymph node numbers, LVI, stage, index year, SMI, and SMD were identified as potential covariates. Patients in G2 (HR=2.446, 95% CI=1.650–3.628, P<0.001), G3 (HR=2.223, 95% CI=1.453–3.401, P<0.001), and G4 (HR=3.702, 95% CI=2.223–6.163, P<0.001) had significantly lower OS rates compared to those of patients in G1. In the multivariable analysis, poor OS was observed in patients in G2 (HR=1.676, 95% CI=1.110–2.529, P=0.013), G3 (HR=1.916, 95% CI=1.249–2.938, P=0.002), and G4 (HR=2.172, 95% CI=1.279–3.687, P=0.004) compared to those of patients in G1 after adjusting for potential covariates (Table 3).
A C-index comparison revealed that grouping patients into the combined group was a better prognostic factor for OS in patients with CRC than SMI (CI difference=0.062, 95% CI=0.031–0.103, P=0.0011) or creatinine level (CI difference=0.043, 95% CI=0.017–0.081, P=0.0072) alone (Table 4).
Discussion
Our study demonstrated that combining SMI and creatinine level for subgrouping was more effective in predicting OS for patients with CRC than using SMI alone to classify sarcopenia. Interestingly, even among individuals without sarcopenia, differences in OS were observed between those with high and those with low creatinine levels. Additionally, no significant difference was observed in the OS rates between patients without sarcopenia with high creatinine levels and patients with sarcopenia. Consequently, integrating preoperative creatinine levels with SMI could greatly improve prognostic stratification, surpassing the predictive capability of solely assessing the presence or absence of sarcopenia when evaluating OS in patients with non-metastatic CRC.
Previous studies have suggested using sarcopenia as a predictive tool for evaluating the prognosis of patients with cancer, including those with CRC. However, conflicting findings have emerged, raising doubts about the reliability of sarcopenia as an indicator of prognosis [13-15]. One of the reasons behind this uncertainty is the diagnostic criteria for sarcopenia, which are predominantly based on standards derived from studies conducted on Western populations [11]. Since muscle mass can vary among racial or ethnic groups, using cut-off values from Western populations may not be suitable for other ethnic groups. Consequently, researchers established and applied new standard values tailored to their study group [16]. Nevertheless, differing standard values is a significant drawback because it limits comparability of studies. These challenges should be considered while adopting CT-based sarcopenia as a diagnostic criterion.
Ongoing studies indicated that creatinine may serve as an indicator of muscle mass; however, only a few studies have assessed the association between serum creatinine level and SMI [17-21]. Since SMI is a direct measurement of skeletal muscle area and creatinine level is also linked to skeletal muscle, one can reasonably speculate on a potential correlation between these two factors. However, when analyzing actual patient data in our study, we observed no association between SMI and creatinine levels in males, although a positive correlation was observed in females. The reason for this discrepancy, particularly with more pronounced changes in SMI and creatinine levels in females with relatively early stage CRC, remains unclear. Although creatinine production might be proportional to muscle mass, serum creatinine level is also influenced by renal function decline. Therefore, incorporating cystatin C level, which can reflect GFR, may provide a more accurate reflection of renal function [22]. Some studies have explored the relationship between SMI and the serum creatinine to cystatin C ratio, rather than relying solely on serum creatinine. For instance, in one study, researchers found a significant correlation between weight-adjusted serum creatinine to cystatin C ratio and weight-adjusted SMI in both males (r=0.484, P<0.001) and females (r=0.538, P<0.001) [23]. It is important to acknowledge the limitations of our study, wherein cystatin C levels could not be confirmed. Further research is required to determine whether variables, including cystatin C, can accurately reflect skeletal muscle mass.
Building upon this knowledge, our study aimed to assess the prognosis of patients with CRC by categorizing them according to SMI level and serum creatinine level. Previous studies have evaluated the association between serum creatinine level and OS in various types of cancer [24-26]. In particular, a multi-center cohort study analyzing the association between serum creatinine level and OS in patients with CRC categorized the patients into three groups based on serum creatinine level. In that study, patients were assigned into the low serum creatinine group (<0.80 mg/dL in males or <0.67 mg/dL in females), the normal serum creatinine group (0.80–1.18 mg/dL in males or 0.67–0.96 mg/dL in females), and the high serum creatinine group (>1.18 mg/dL in males or >0.96 mg/dL in females), where the normal range was determined based on the central 95th percentile of serum creatinine distribution in healthy individuals. These cutoff values were not tailored specifically to patients with CRC, suggesting that they may not be the most appropriate indicators for assessing CRC in patients [24,27]. In contrast, in this present investigation, novel threshold values for serum creatinine level were established for the CRC patient cohort using the X-tile program, with values of 1.01 mg/dL for males and 0.80 mg/dL for females. These values were obtained considering the OS in patients with CRC, with the aim of finding predictive values for prognosis. Furthermore, because it is easy to examine serum creatinine and complete blood count with low cost, this high-accessibility method would be more advantageous for predicting the OS of patients with CRC.
The potential utility of creatinine as an indicator closely associated with sarcopenia, reflecting changes in muscle mass, appears plausible. It is worth considering that individuals with higher creatinine levels may have a less favorable prognosis, particularly in patients in whom significant skeletal muscle mass reduction may not be evident but is in its earlier stage. Therefore, our research suggested an approach for identifying patients whose skeletal muscle area may not adequately reflect their sarcopenic status, aiding in identification of this specific patient subset.
Our study had several limitations. First, the present study was conducted at a single center, which might restrict the applicability of our findings to a broader population and might decrease the universal applicability of the devised threshold of serum creatinine level. To enhance the external validity and improve the accuracy of our analysis, future research should include a multicenter study involving diverse patient cohorts. Second, we focused solely on 5-year OS in our evaluation of outcomes. To provide a more comprehensive prognostic value, future investigations should incorporate other significant endpoints, such as postoperative complications or quality of life. Finally, we did not systematically assess potential confounding factors, including chronic renal disease, low eGFR, or local infections, which could potentially influence serum creatinine level. The presence of these factors may have introduced bias, and concerns about potential inclusion of renal failure patients in the high serum creatinine group was not fully eliminated. Therefore, future studies should consider these confounding variables to strengthen the validity of the findings.
Our study demonstrated that combining SMI and serum creatinine level was a more effective approach for predicting OS in patients with CRC compared to using SMI alone to assess sarcopenia. Sarcopenia has been identified as a factor influencing OS in various cancer types, and the inclusion of serum creatinine level enhances the prognostic value, specifically for patients with CRC, beyond the use of SMI or creatinine level alone in current clinical practice. By addressing the limitations of existing standards, our research provides a more robust and reliable prognostic indicator for patients with CRC.
Supplementary materials
Supplementary materials can be found via https://doi.org/10.15747/ACNM.2024.16.2.66
Supplement 1. Cut-off values of creatinine based on sex using the X-tile program.
Acknowledgements
None.
Authors’ contribution
Conceptualization: JC, JK. Data curation: HSL, JK. Formal analysis: HSL. Funding acquisition: JK. Investigation: HSL, JK. Methodology: JC, JK. Project administration: JK, JK. Resources: HSL, JK. Software: JC, HSL. Supervision: JK. Validation: JK. Visualization: JC. Writing – original draft: JC. Writing – review & editing: JC, JK.
Conflict of interest
The authors of this manuscript have no conflicts of interest to disclose.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1F1A1074811).
Data availabity
Due to the retrospective nature of this study and the utilization of patient data, we do not have ethical approval to publish the raw data or transfer it from our hospital electronic medical server.
Fig. 1
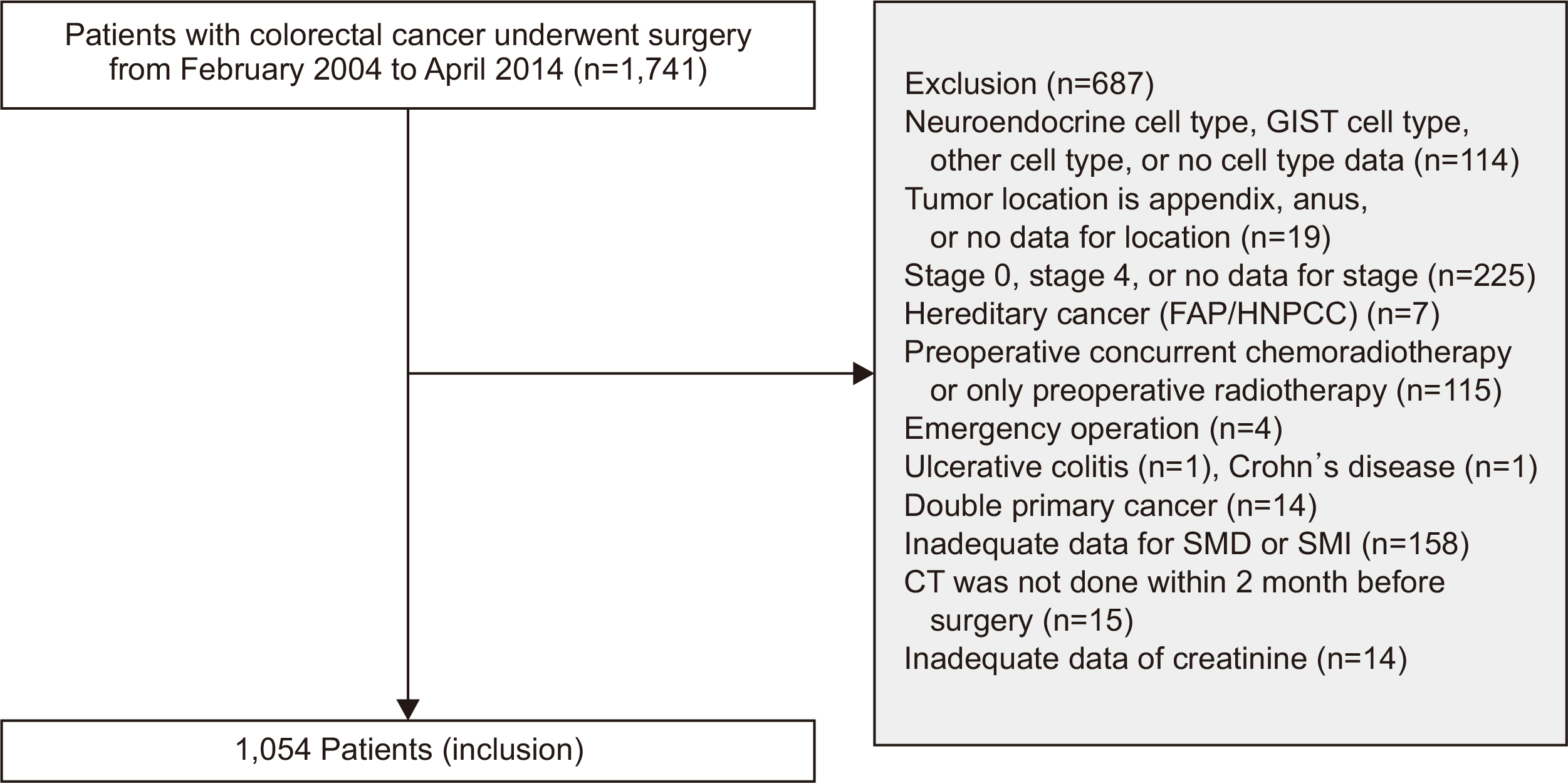
Inclusion criteria. GIST = gastrointestinal stromal tumor; FAP/HNPCC = familial adenomatous polyposis/hereditary nonpolyposis colorectal cancer; SMD = skeletal muscle radiodensity; SMI = skeletal muscle index; CT = computed tomography.
Fig. 2
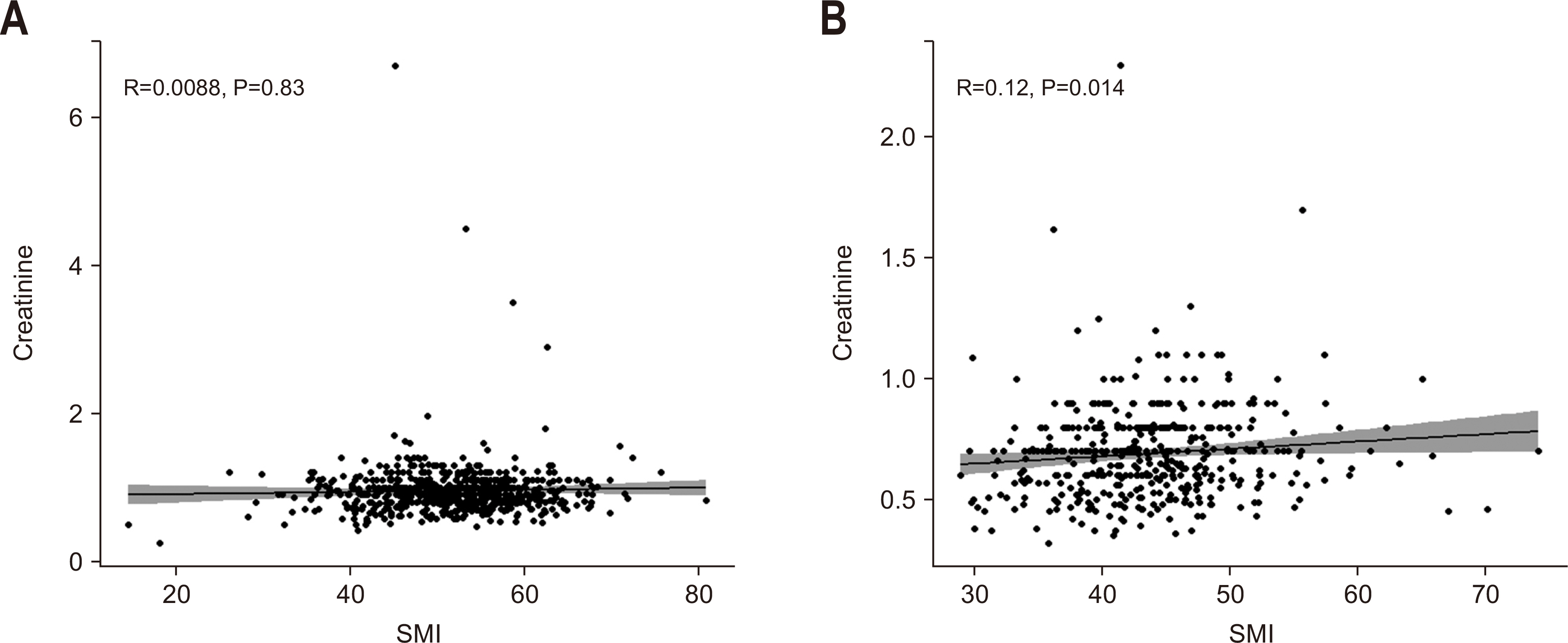
Spearman’s rank correlation test between skeletal muscle index (SMI) and creatinine level for males (A) and females (B).
Fig. 3
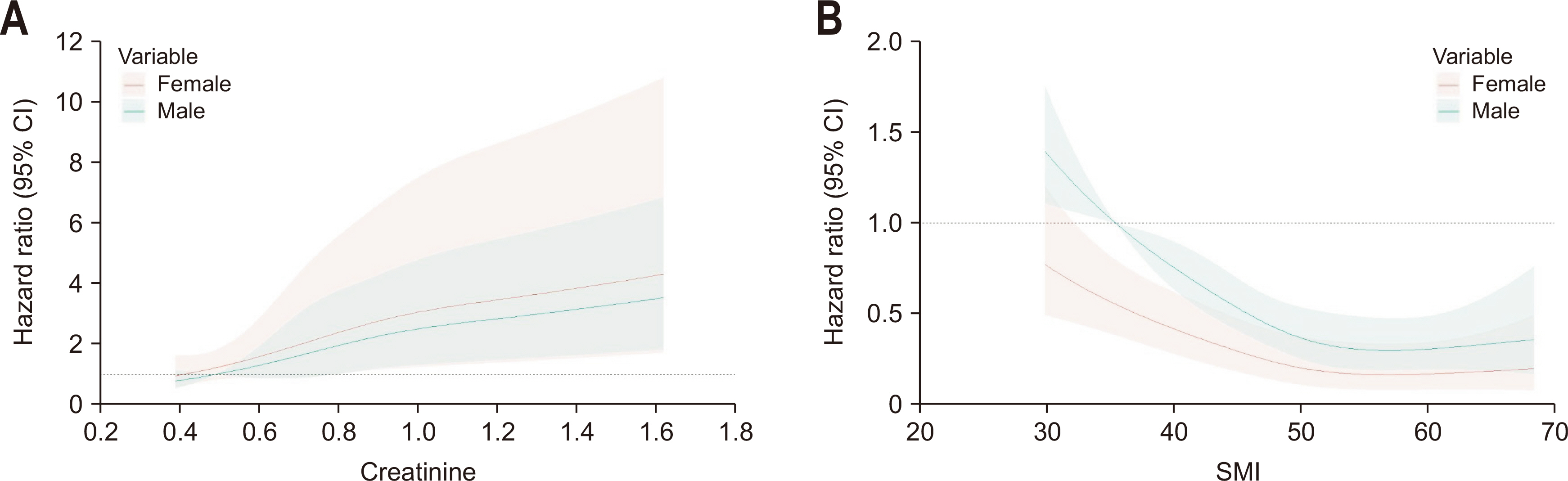
Association between creatinine and skeletal muscle index (SMI) and overall survival according to sex using a restricted cubic spline regression model. Graphs show hazard ratios for overall survival according to creatinine (A) and SMI (B) of each sex adjusted for sex. Data were fitted by a restricted cubic spline Cox proportional hazards regression model, and the model was conducted with 4 knots at the 5th, 35th, 65th, and 95th percentiles of creatinine and SMI (reference is the 5th percentile). Solid lines indicate hazard ratios, and shadow shape indicates the 95% confidence interval (CI).
Fig. 4
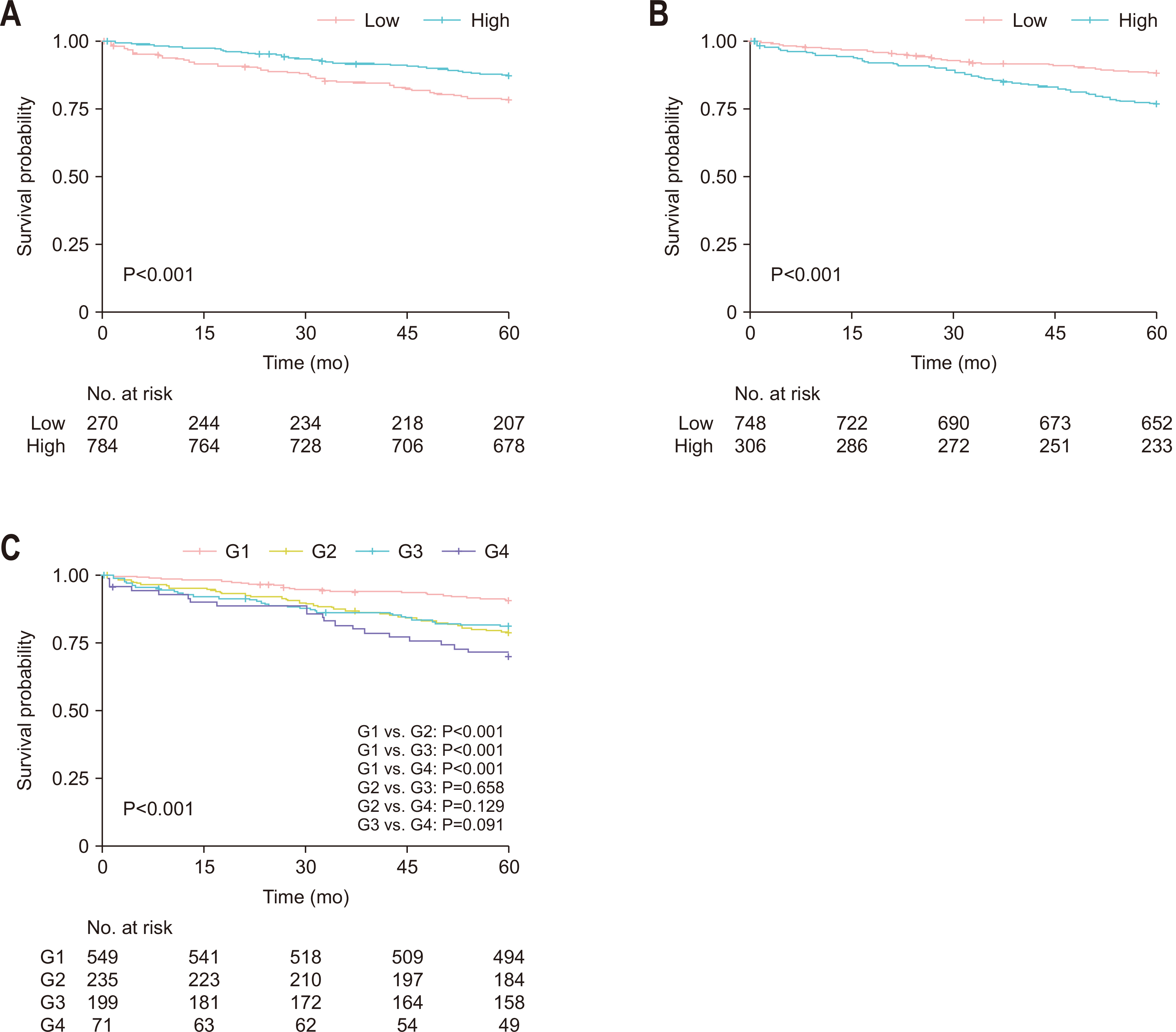
Kaplan-Meier survival curve of overall survival. (A) Skeletal muscle index (SMI). (B) Creatinine. (C) Combined classification. G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; G4 = sarcopenia with high serum creatinine level.
Fig. 5
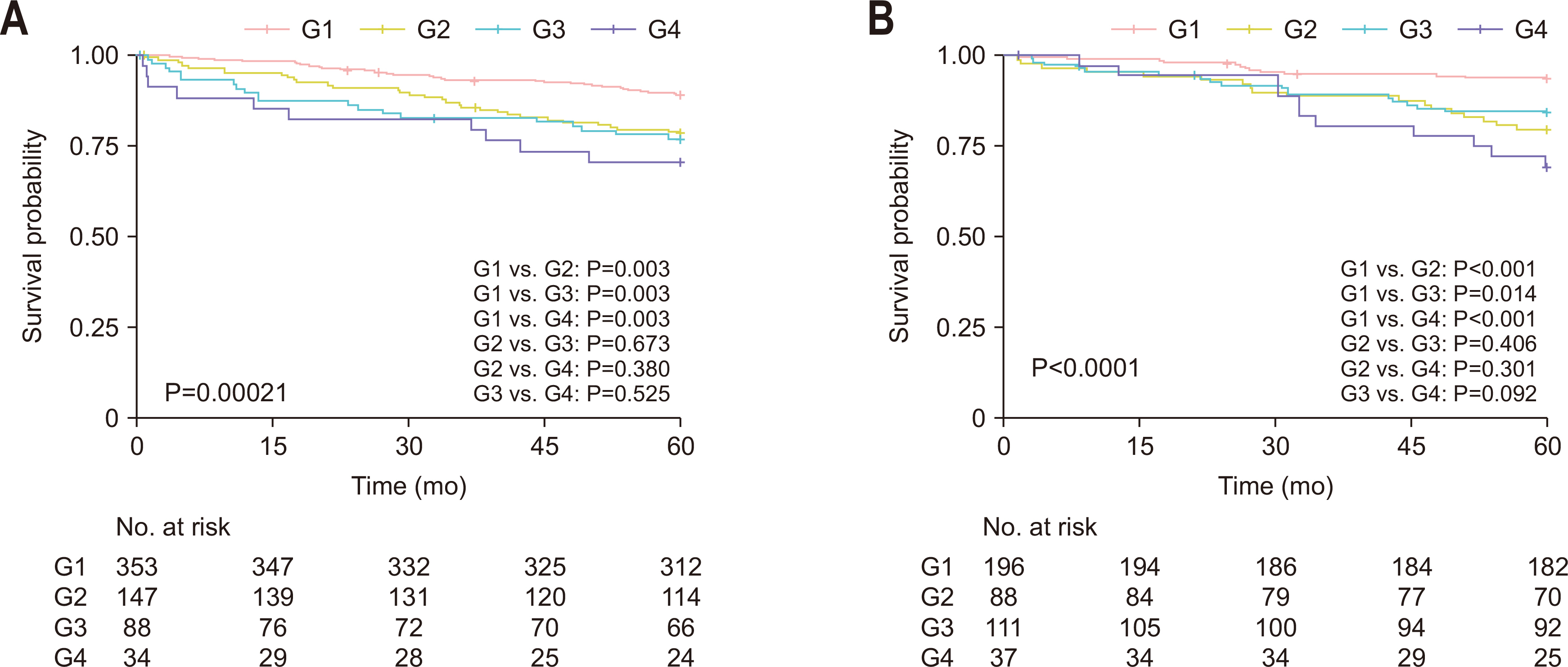
Kaplan-Meier survival curve based on the combined groups according to sex. (A) Male. (B) Female. G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; G4 = sarcopenia with high serum creatinine level.
Table 1
Patient characteristics according to the skeletal muscle index and serum creatinine level
Values are presented as number (%) or mean±standard deviation.
SMI = skeletal muscle index; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; LVI = lymphovascular invasion; SMD = skeletal muscle radiodensity; HU = Hounsfield unit.
Table 2
Univariate analysis of factors associated with overall survival
HR = hazard ratio; CI = confidence interval; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; LVI = lymphovascular invasion; SMI = skeletal muscle index; SMD = skeletal muscle radiodensity; HU = Hounsfield unit; G4 = sarcopenia with high serum creatinine level.
Table 3
Multivariable analysis of factors associated with overall survival
HR = hazard ratio; CI = confidence interval; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; SMD = skeletal muscle radiodensity; HU = Hounsfield unit; G4 = sarcopenia with high serum creatinine level.
Table 4
Comparison of C-index between combined group and skeletal muscle index or serum creatinine alone
- 1. Baidoun F, Elshiwy K, Elkeraie Y, Merjaneh Z, Khoudari G, Sarmini MT, et al. Colorectal cancer epidemiology: recent trends and impact on outcomes. Curr Drug Targets 2021;22:998-1009. ArticlePubMed
- 2. Kang MJ, Jung KW, Bang SH, Choi SH, Park EH, Yun EH, et al. Community of Population-Based Regional Cancer Registries. Cancer Statistics in Korea: incidence, mortality, survival, and prevalence in 2020. Cancer Res Treat 2023;55:385-99. ArticlePubMedPMCPDF
- 3. Ubachs J, Ziemons J, Minis-Rutten IJG, Kruitwagen RFPM, Kleijnen J, Lambrechts S, et al. Sarcopenia and ovarian cancer survival: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle 2019;10:1165-74. ArticlePubMedPMCPDF
- 4. Feliciano EMC, Kroenke CH, Meyerhardt JA, Prado CM, Bradshaw PT, Kwan ML, et al. Association of systemic inflammation and sarcopenia with survival in nonmetastatic colorectal cancer: results from the C SCANS Study. JAMA Oncol 2017;3:e172319. ArticlePubMedPMC
- 5. Jogiat UM, Bédard ELR, Sasewich H, Turner SR, Eurich DT, Filafilo H, et al. 2022;Sarcopenia reduces overall survival in unresectable oesophageal cancer: a systematic review and meta-analysis. J Cachexia Sarcopenia Muscle 13:2630-6. ArticlePubMedPMCPDF
- 6. Kashani K, Rosner MH, Ostermann M. Creatinine: from physiology to clinical application. Eur J Intern Med 2020;72:9-14. ArticlePubMed
- 7. Dudani S, Marginean H, Gotfrit J, Tang PA, Monzon JG, Dennis K, et al. The impact of chronic kidney disease in patients with locally advanced rectal cancer treated with neoadjuvant chemoradiation. Dis Colon Rectum 2021;64:1471-8. ArticlePubMedPMC
- 8. Obara S, Koyama F, Kuge H, Nakamoto T, Ikeda N, Iwasa Y, et al. Effect of preoperative asymptomatic renal dysfunction on the clinical course after colectomy for colon cancer. Surg Today 2022;52:106-13. ArticlePubMedPDF
- 9. Chan JCY, Diakos CI, Engel A, Chan DLH, Pavlakis N, Gill A, et al. Serum bicarbonate is a marker of peri-operative mortality but is not associated with long term survival in colorectal cancer. PLoS One 2020;15:e0228466. ArticlePubMedPMC
- 10. Watanabe A, Oshikiri T, Sawada R, Harada H, Urakawa N, Goto H, et al. 2022;Actual sarcopenia reflects poor prognosis in patients with esophageal cancer. Ann Surg Oncol 29:3670-81. ArticlePubMedPDF
- 11. Martin L, Birdsell L, Macdonald N, Reiman T, Clandinin MT, McCargar LJ, et al. Cancer cachexia in the age of obesity: skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J Clin Oncol 2013;31:1539-47. ArticlePubMed
- 12. Camp RL, Dolled-Filhart M, Rimm DL. X-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin Cancer Res 2004;10:7252-9. PubMed
- 13. Oh RK, Ko HM, Lee JE, Lee KH, Kim JY, Kim JS. Clinical impact of sarcopenia in patients with colon cancer undergoing laparoscopic surgery. Ann Surg Treat Res 2020;99:153-60. ArticlePubMedPMCPDF
- 14. van Vugt JLA, Coebergh van den Braak RRJ, Lalmahomed ZS, Vrijland WW, Dekker JWT, Zimmerman DDE, et al. Impact of low skeletal muscle mass and density on short and long-term outcome after resection of stage I-III colorectal cancer. Eur J Surg Oncol 2018;44:1354-60. ArticlePubMed
- 15. Han JS, Ryu H, Park IJ, Kim KW, Shin Y, Kim SO, et al. Association of body composition with long-term survival in non-metastatic rectal cancer patients. Cancer Res Treat 2020;52:563-72. ArticlePubMedPDF
- 16. McGovern J, Dolan RD, Horgan PG, Laird BJ, McMillan DC. Computed tomography-defined low skeletal muscle index and density in cancer patients: observations from a systematic review. J Cachexia Sarcopenia Muscle 2021;12:1408-17. ArticlePubMedPMCPDF
- 17. Delgado C, Johansen KL. Revisiting serum creatinine as an indicator of muscle mass and a predictor of mortality among patients on hemodialysis. Nephrol Dial Transplant 2020;35:2033-5. ArticlePubMedPMCPDF
- 18. Yamada S, Arase H, Taniguchi M, Kitazono T, Nakano T. Comparison of the predictability of serum creatinine-based surrogates of skeletal muscle mass for all-cause mortality in patients receiving hemodialysis: creatinine generation rate and creatinine index. Clin Exp Nephrol 2022;26:488-9. ArticlePubMedPDF
- 19. Kim SW, Jung HW, Kim CH, Kim KI, Chin HJ, Lee H. A new equation to estimate muscle mass from creatinine and cystatin C. PLoS One 2016;11:e0148495. ArticlePubMedPMC
- 20. Patel SS, Molnar MZ, Tayek JA, Ix JH, Noori N, Benner D, et al. 2013;Serum creatinine as a marker of muscle mass in chronic kidney disease: results of a cross-sectional study and review of literature. J Cachexia Sarcopenia Muscle 4:19-29. ArticlePubMed
- 21. das Neves W, Alves CRR, de Souza Borges AP, de Castro G Jr. Serum creatinine as a potential biomarker of skeletal muscle atrophy in non-small cell lung cancer patients. Front Physiol 2021;12:625417. PubMedPMC
- 22. Tabara Y, Okada Y, Ochi M, Ohyagi Y, Igase M. 2021;Different associations of skeletal muscle mass index and creatinine-to-cystatin C ratio with muscle mass and myosteatosis: the J-SHIPP study. J Am Med Dir Assoc 22:2600-2. ArticlePubMed
- 23. Nishida K, Hashimoto Y, Kaji A, Okamura T, Sakai R, Kitagawa N, et al. Creatinine/(cystatin C × body weight) ratio is associated with skeletal muscle mass index. Endocr J 2020;67:733-40. ArticlePubMed
- 24. Yang M, Zhang Q, Ruan GT, Tang M, Zhang X, Song MM, et al. Association between serum creatinine concentrations and overall survival in patients with colorectal cancer: a multi-center cohort study. Front Oncol 2021;11:710423. ArticlePubMedPMC
- 25. Lafleur J, Hefler-Frischmuth K, Grimm C, Schwameis R, Gensthaler L, Reiser E, et al. 2018;Prognostic value of serum creatinine levels in patients with epithelial ovarian cancer. Anticancer Res 38:5127-30. ArticlePubMed
- 26. Schwameis R, Postl M, Bekos C, Hefler L, Reinthaller A, Seebacher V, et al. Prognostic value of serum creatine level in patients with vulvar cancer. Sci Rep 2019;9:11129. ArticlePubMedPMCPDF
- 27. Li H, Zhang X, Xu G, Wang X, Zhang C. 2009;Determination of reference intervals for creatinine and evaluation of creatinine-based estimating equation for Chinese patients with chronic kidney disease. Clin Chim Acta 403:87-91. ArticlePubMed
References
Figure & Data
REFERENCES
Citations
Citations to this article as recorded by 
 ePub Link
ePub Link Cite
CitePrognostic significance of serum creatinine and sarcopenia for 5-year overall survival in patients with colorectal cancer in Korea: a comparative study
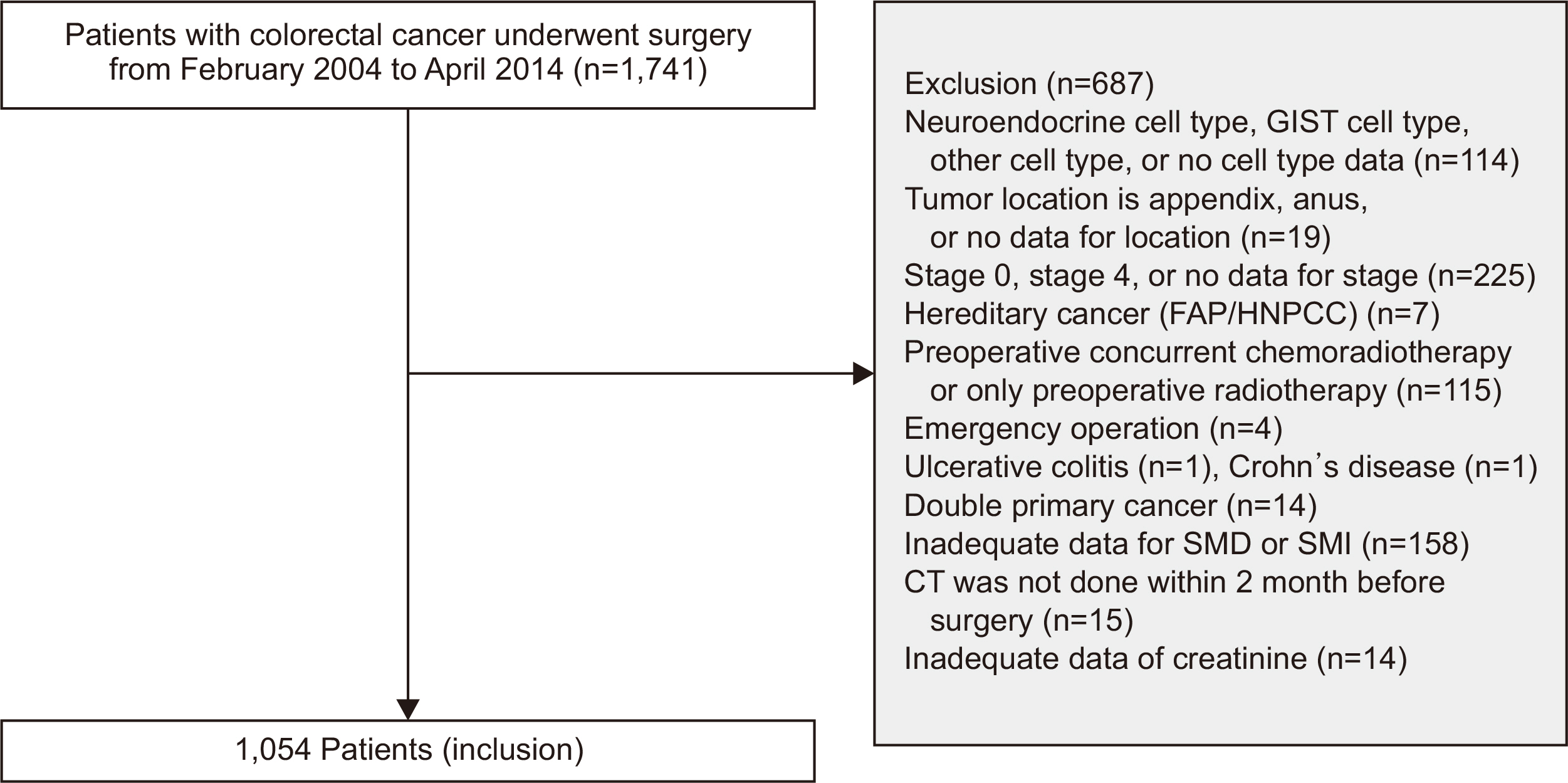
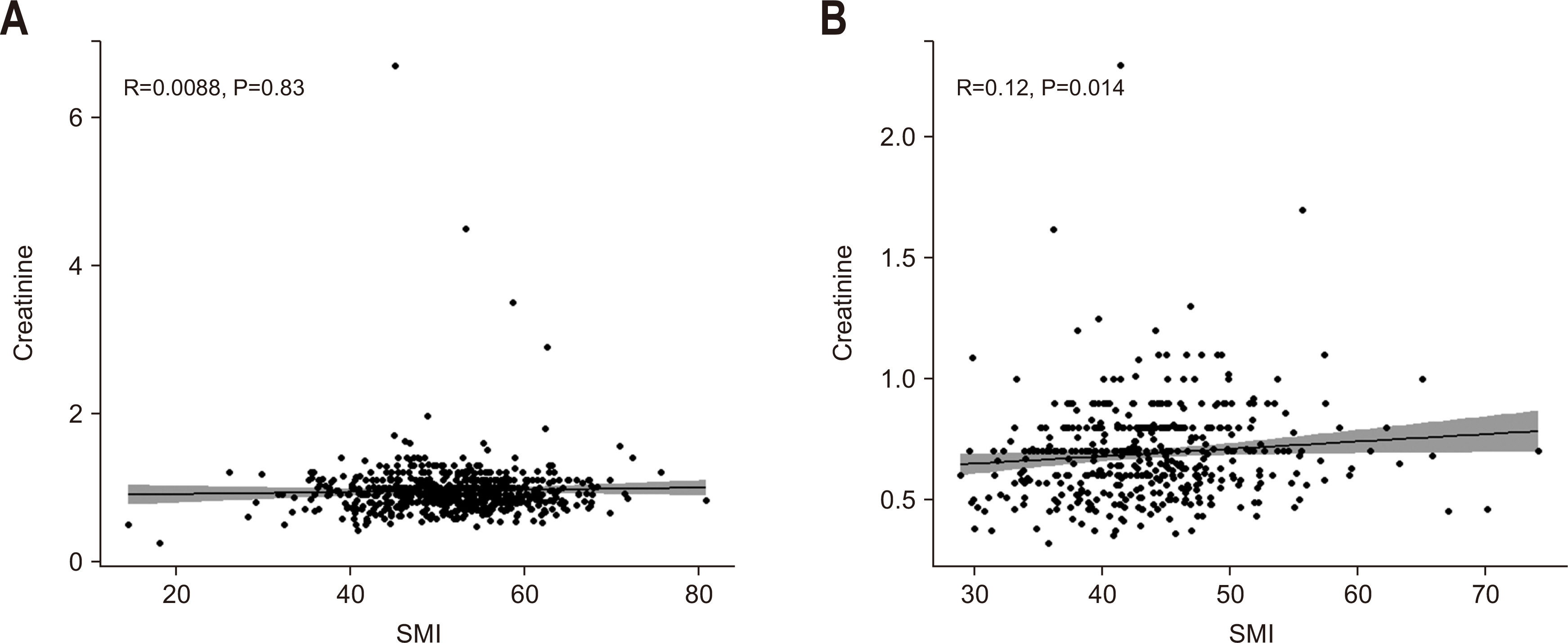
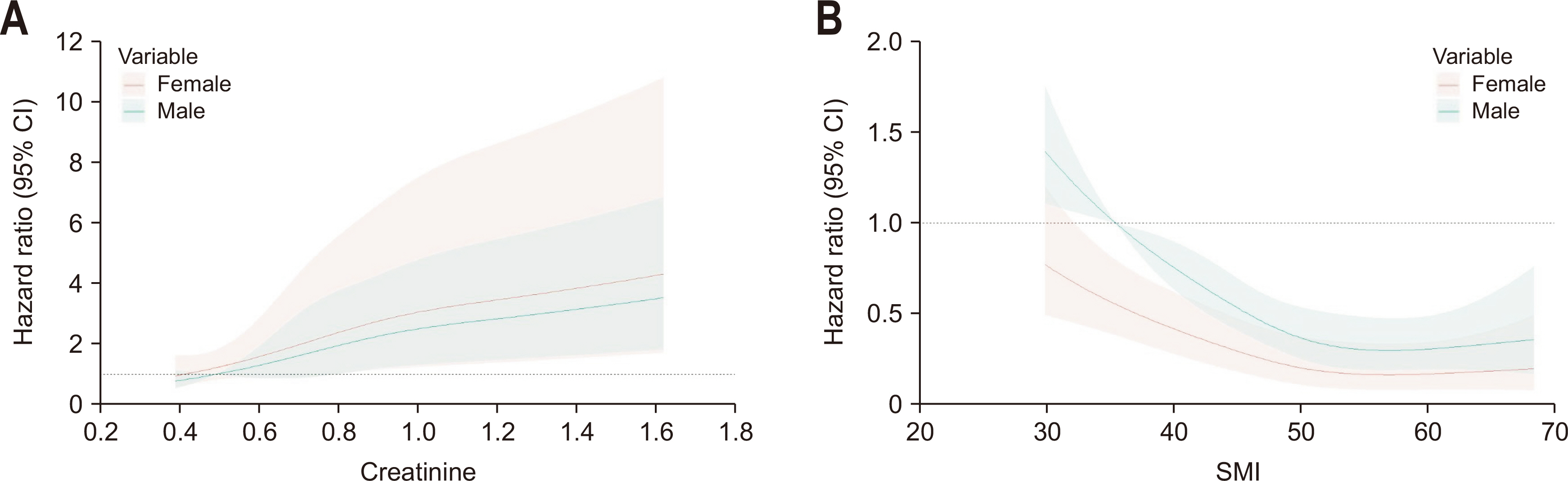
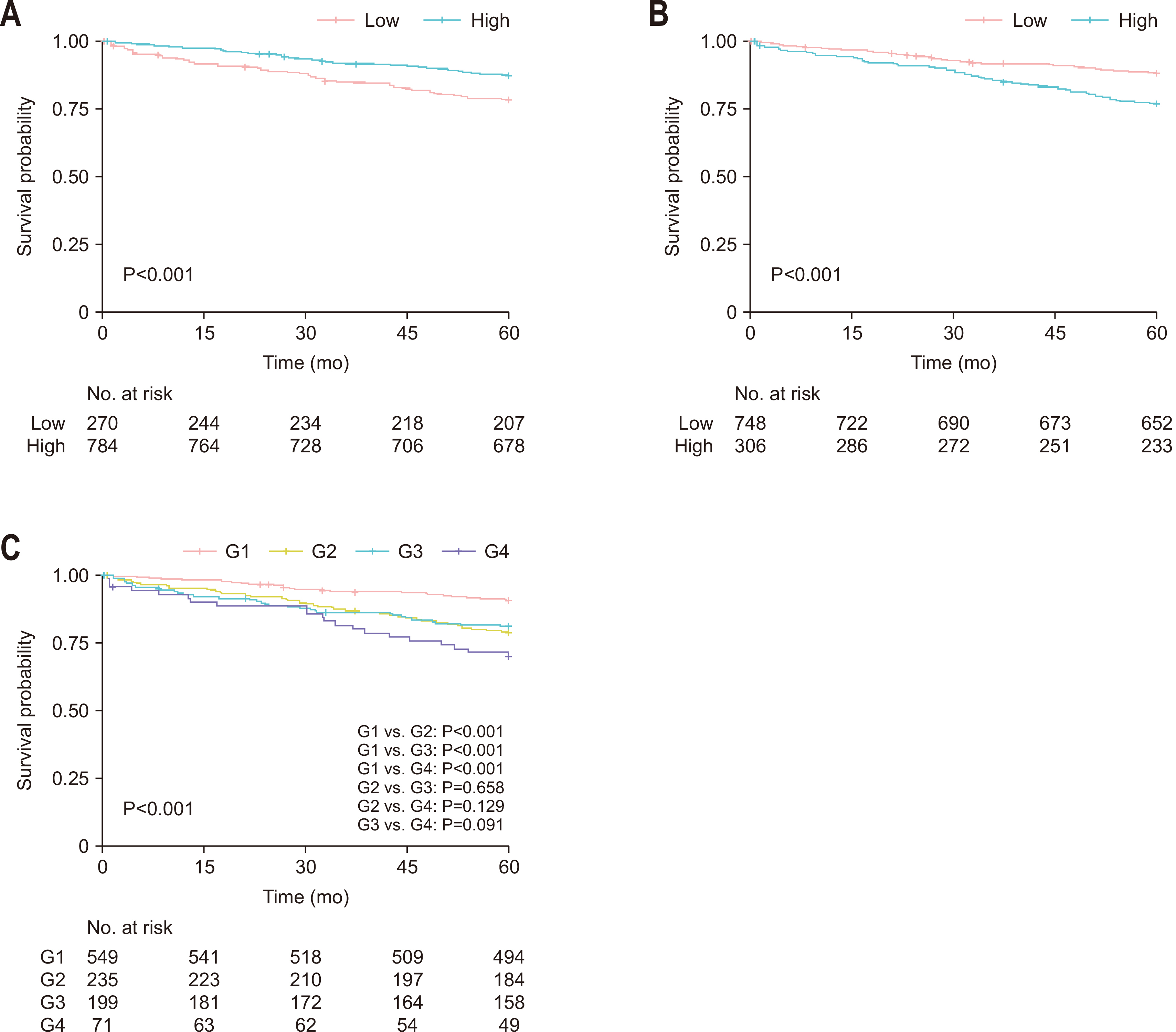
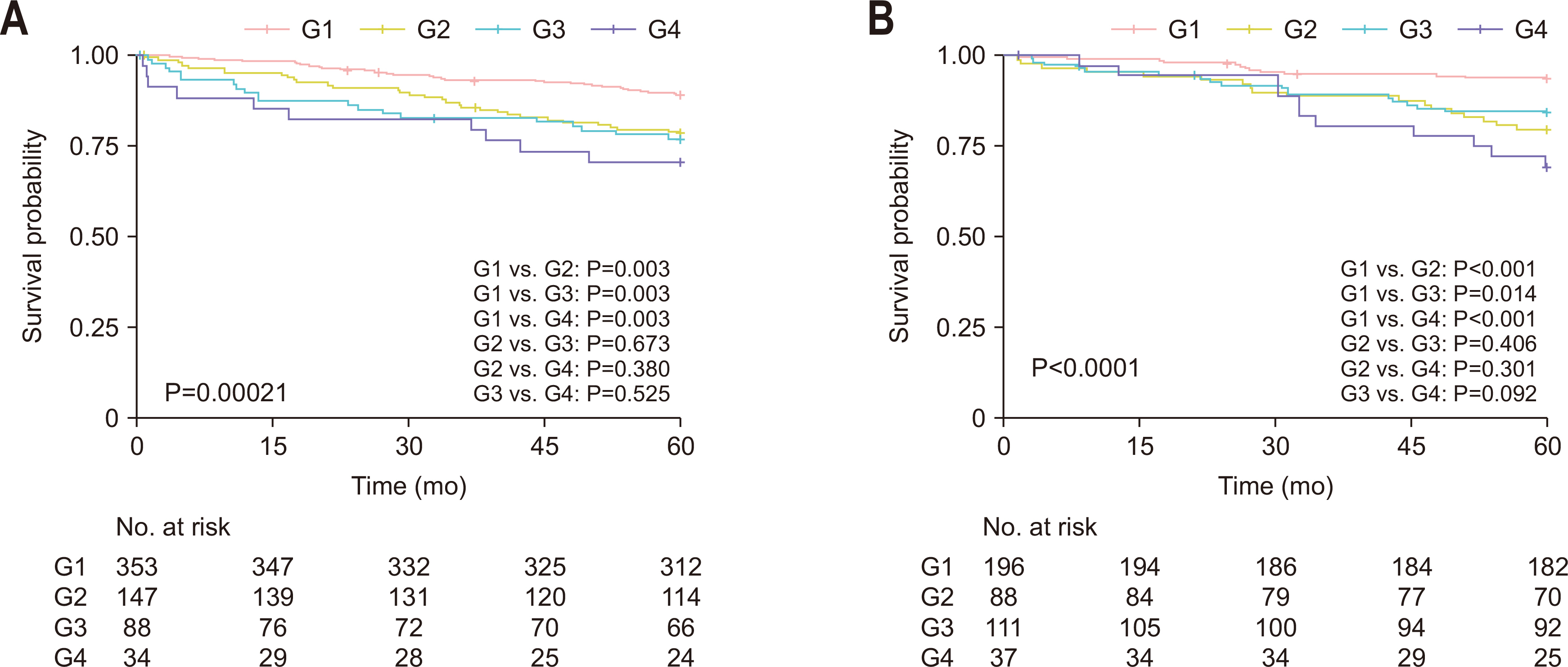
Fig. 1
Inclusion criteria. GIST = gastrointestinal stromal tumor; FAP/HNPCC = familial adenomatous polyposis/hereditary nonpolyposis colorectal cancer; SMD = skeletal muscle radiodensity; SMI = skeletal muscle index; CT = computed tomography.
Fig. 2
Spearman’s rank correlation test between skeletal muscle index (SMI) and creatinine level for males (A) and females (B).
Fig. 3
Association between creatinine and skeletal muscle index (SMI) and overall survival according to sex using a restricted cubic spline regression model. Graphs show hazard ratios for overall survival according to creatinine (A) and SMI (B) of each sex adjusted for sex. Data were fitted by a restricted cubic spline Cox proportional hazards regression model, and the model was conducted with 4 knots at the 5th, 35th, 65th, and 95th percentiles of creatinine and SMI (reference is the 5th percentile). Solid lines indicate hazard ratios, and shadow shape indicates the 95% confidence interval (CI).
Fig. 4
Kaplan-Meier survival curve of overall survival. (A) Skeletal muscle index (SMI). (B) Creatinine. (C) Combined classification. G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; G4 = sarcopenia with high serum creatinine level.
Fig. 5
Kaplan-Meier survival curve based on the combined groups according to sex. (A) Male. (B) Female. G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; G4 = sarcopenia with high serum creatinine level.
Fig. 1
Fig. 2
Fig. 3
Fig. 4
Fig. 5
Prognostic significance of serum creatinine and sarcopenia for 5-year overall survival in patients with colorectal cancer in Korea: a comparative study
Patient characteristics according to the skeletal muscle index and serum creatinine level
| Variable | Categorization | Low SMI (n=270) | High SMI (n=784) | P-value | Low creatinine (n=748) | High creatinine (n=306) | P-value |
|---|---|---|---|---|---|---|---|
| Sex | Female | 148 (54.8) | 284 (36.2) | 307 (41.0) | 125 (40.8) | ||
| Male | 122 (45.2) | 500 (63.8) | <0.001 | 441 (59.0) | 181 (59.2) | >0.999 | |
| Age (yr) | <70 | 168 (62.2) | 545 (69.5) | 546 (73.0) | 167 (54.6) | ||
| ≥70 | 102 (37.8) | 239 (30.5) | 0.033 | 202 (27.0) | 139 (45.4) | <0.001 | |
| Diabetes mellitus | No | 226 (83.7) | 625 (79.7) | 622 (83.2) | 229 (74.8) | ||
| Yes | 44 (16.3) | 159 (20.3) | 0.179 | 126 (16.8) | 77 (25.2) | 0.003 | |
| Hypertension | No | 168 (62.2) | 436 (55.6) | 469 (62.7) | 135 (44.1) | ||
| Yes | 102 (37.8) | 348 (44.4) | 0.068 | 279 (37.3) | 171 (55.9) | <0.001 | |
| Smoking | No | 198 (73.3) | 528 (67.3) | 508 (67.9) | 218 (71.2) | ||
| Yes | 72 (26.7) | 256 (32.7) | 0.079 | 240 (32.1) | 88 (28.8) | 0.324 | |
| BMI (kg/m2) | 21.8±3.2 | 24.1±2.8 | <0.001 | 23.4±3.0 | 23.7±3.2 | 0.226 | |
| CEA (ng/mL) | <5 | 181 (67.0) | 548 (69.9) | 515 (68.9) | 214 (69.9) | ||
| ≥5 | 75 (27.8) | 202 (25.8) | 193 (25.8) | 84 (27.5) | |||
| Unknown | 14 (5.2) | 34 (4.3) | 0.649 | 40 (5.3) | 8 (2.6) | 0.148 | |
| Tumor location | Colon | 201 (74.4) | 534 (68.1) | 528 (70.6) | 207 (67.6) | ||
| Rectum | 69 (25.6) | 250 (31.9) | 0.061 | 220 (29.4) | 99 (32.4) | 0.385 | |
| Histologic grade | G1 & G2 | 249 (92.2) | 723 (92.2) | 691 (92.4) | 281 (91.8) | ||
| G3 & MC & SRC | 21 (7.8) | 61 (7.8) | >0.99 | 57 (7.6) | 25 (8.2) | 0.861 | |
| LVI | Absent | 181 (67.0) | 550 (70.2) | 524 (70.1) | 207 (67.6) | ||
| Present | 58 (21.5) | 157 (20.0) | 152 (20.3) | 63 (20.6) | |||
| Unknown | 31 (11.5) | 77 (9.8) | 0.597 | 72 (9.6) | 36 (11.8) | 0.560 | |
| Lymph nodes | <12 | 39 (14.4) | 125 (15.9) | 90 (12.0) | 74 (24.2) | ||
| ≥12 | 231 (85.6) | 659 (84.1) | 0.625 | 658 (88.0) | 232 (75.8) | <0.001 | |
| Stage | I | 56 (20.7) | 213 (27.2) | 201 (26.9) | 68 (22.2) | ||
| II | 96 (35.6) | 252 (32.1) | 248 (33.2) | 100 (32.7) | |||
| III | 118 (43.7) | 319 (40.7) | 0.111 | 299 (40.0) | 138 (45.1) | 0.199 | |
| Complications | No | 206 (76.3) | 608 (77.6) | 598 (79.9) | 216 (70.6) | ||
| Yes | 64 (23.7) | 176 (22.4) | 0.734 | 150 (20.1) | 90 (29.4) | 0.001 | |
| Chemotherapy | No | 124 (45.9) | 302 (38.5) | 316 (42.2) | 110 (35.9) | ||
| Yes | 146 (54.1) | 482 (61.5) | 0.039 | 432 (57.8) | 196 (64.1) | 0.068 | |
| Index year | 2006–2009 | 113 (41.9) | 329 (42.0) | 250 (33.4) | 192 (62.7) | ||
| 2010–2014 | 157 (58.1) | 455 (58.0) | >0.99 | 498 (66.6) | 114 (37.3) | <0.001 | |
| Creatinine (mg/dL) | 0.8±0.2 | 0.9±0.4 | <0.001 | 0.7±0.2 | 1.1±0.5 | <0.001 | |
| SMI (cm2/m2) | 39.1±5.6 | 51.7±7.0 | <0.001 | 48.2±8.7 | 49.0±8.4 | 0.189 | |
| SMD (HU) | 41.0±8.7 | 42.8±8.4 | 0.004 | 42.6±8.3 | 41.5±8.9 | 0.054 |
Values are presented as number (%) or mean±standard deviation.
SMI = skeletal muscle index; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; LVI = lymphovascular invasion; SMD = skeletal muscle radiodensity; HU = Hounsfield unit.
Univariate analysis of factors associated with overall survival
| Variable | Categorization | Univariate analysis | |
|---|---|---|---|
| HR (95% CI) | P-value | ||
| Sex | Female | 1 | |
| Male | 1.205 (0.871–1.666) | 0.26 | |
| Age (yr) | <70 | 1 | |
| ≥70 | 2.592 (1.895–3.546) | <0.001 | |
| Diabetes mellitus | No | 1 | |
| Yes | 1.041 (0.702–1.541) | 0.843 | |
| Hypertension | No | 1 | |
| Yes | 1.324 (0.968–1.811) | 0.078 | |
| Smoking | No | 1 | |
| Yes | 0.940 (0.668–1.323) | 0.725 | |
| BMI (kg/m2) | <25 | 1 | |
| ≥25 | 0.575 (0.390–0.848) | 0.005 | |
| CEA (ng/mL) | <5 | 1 | |
| ≥5 | 2.012 (1.456–2.781) | <0.001 | |
| Unknown | 1.044 (0.456–2.386) | 0.919 | |
| Tumor location | Colon | 1 | |
| Rectum | 0.913 (0.646–1.291) | 0.608 | |
| Complications | No | 1 | |
| Yes | 1.91 (1.372–2.658) | <0.001 | |
| Histologic grade | G1 & G2 | 1 | |
| G3 & MC & SRC | 2.114 (1.347–3.317) | 0.001 | |
| LVI | Absent | 1 | |
| Present | 2.197 (1.559–3.096) | <0.001 | |
| Unknown | 1.331 (0.791–2.237) | 0.281 | |
| Lymph nodes | <12 | 1 | |
| ≥12 | 0.657 (0.450–0.961) | 0.03 | |
| Stage | I | 1 | |
| II | 2.316 (1.287–4.169) | 0.005 | |
| III | 4.528 (2.630–7.795) | <0.001 | |
| Chemotherapy | No | 1 | |
| Yes | 0.859 (0.626–1.179) | 0.347 | |
| Index year | 2006–2009 | 1 | |
| 2010–2014 | 0.573 (0.419–0.785) | <0.001 | |
| SMI (cm2/m2) | Low | 1 | |
| High | 0.544 (0.393–0.752) | <0.001 | |
| SMD (HU) | Low | 1 | |
| High | 0.384 (0.281–0.525) | <0.001 | |
| Creatinine (mg/dL) | Low | 1 | |
| High | 2.086 (1.523–2.858) | <0.001 | |
| Combined groups | G1 | 1 | |
| G2 | 2.446 (1.650–3.628) | <0.001 | |
| G3 | 2.223 (1.453–3.401) | <0.001 | |
| G4 | 3.702 (2.223–6.163) | <0.001 | |
HR = hazard ratio; CI = confidence interval; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; LVI = lymphovascular invasion; SMI = skeletal muscle index; SMD = skeletal muscle radiodensity; HU = Hounsfield unit; G4 = sarcopenia with high serum creatinine level.
Multivariable analysis of factors associated with overall survival
| Variable | Categorization | HR (95% CI) | P-value |
|---|---|---|---|
| Age (yr) | <70 | 1 | |
| ≥70 | 1.863 (1.314–2.641) | <0.001 | |
| BMI (kg/m2) | <25 | 1 | |
| ≥25 | 0.643 (0.431–0.958) | 0.030 | |
| CEA (ng/mL) | <5 | 1 | |
| ≥5 | 1.468 (1.048–2.056) | 0.025 | |
| Unknown | 1.824 (0.787–4.227) | 0.160 | |
| Complications | No | 1 | |
| Yes | 1.498 (1.055–2.127) | 0.023 | |
| Histologic grade | G1 & G2 | 1 | |
| G3 & MC & SRC | 1.514 (0.951–2.412) | 0.080 | |
| Lymph nodes | <12 | 1 | |
| ≥12 | 0.511 (0.337–0.773) | 0.001 | |
| Stage | I | 1 | |
| II | 1.606 (0.851–3.028) | 0.143 | |
| III | 3.558 (2.000–6.328) | <0.001 | |
| Index year | 2006–2009 | 1 | |
| 2010–2014 | 0.707 (0.505–0.990) | 0.043 | |
| SMD (HU) | Low | 1 | |
| High | 0.615 (0.435–0.870) | 0.006 | |
| Combined groups | G1 | 1 | |
| G2 | 1.676 (1.110–2.529) | 0.013 | |
| G3 | 1.916 (1.249–2.938) | 0.002 | |
| G4 | 2.172 (1.279–3.687) | 0.004 |
HR = hazard ratio; CI = confidence interval; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; SMD = skeletal muscle radiodensity; HU = Hounsfield unit; G4 = sarcopenia with high serum creatinine level.
Comparison of C-index between combined group and skeletal muscle index or serum creatinine alone
| Included variable | Combined group | SMI | Combined group | Creatinine |
|---|---|---|---|---|
| C-index (95% CI) (bootstrapped) | 0.626 (0.587–0.666) | 0.564 (0.524–0.602) | 0.626 (0.587–0.666) | 0.583 (0.544–0.623) |
| Estimated difference | 0.062 (0.031–0.103) | 0.043 (0.017–0.081) | ||
C-index = Harrell’s concordance index; SMI = skeletal muscle index; CI = confidence interval.
Table 1
Patient characteristics according to the skeletal muscle index and serum creatinine level
Values are presented as number (%) or mean±standard deviation. SMI = skeletal muscle index; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; LVI = lymphovascular invasion; SMD = skeletal muscle radiodensity; HU = Hounsfield unit.
Table 2
Univariate analysis of factors associated with overall survival
HR = hazard ratio; CI = confidence interval; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; LVI = lymphovascular invasion; SMI = skeletal muscle index; SMD = skeletal muscle radiodensity; HU = Hounsfield unit; G4 = sarcopenia with high serum creatinine level.
Table 3
Multivariable analysis of factors associated with overall survival
HR = hazard ratio; CI = confidence interval; BMI = body mass index; CEA = carcinoembryonic antigen; G1 = no sarcopenia with low serum creatinine level; G2 = no sarcopenia with high serum creatinine levels; G3 = sarcopenia with low serum creatinine level; MC = mucinous adenocarcinoma; SRC = signet-ring cell; SMD = skeletal muscle radiodensity; HU = Hounsfield unit; G4 = sarcopenia with high serum creatinine level.
Table 4
Comparison of C-index between combined group and skeletal muscle index or serum creatinine alone
C-index = Harrell’s concordance index; SMI = skeletal muscle index; CI = confidence interval.

