 E-submission
E-submissionIndexed in:
Scopus, KCI, KoreaMed
Scopus, KCI, KoreaMed

Current issue
- Page Path
- HOME > Browse articles > Current issue
- Volume 18 (1); April 2026
-


Editorial
- Adapting Enhanced Recovery After Surgery for hepatobiliary and pancreatic surgery: a Korean perspective
-
Sang Hyun Shin
- Ann Clin Nutr Metab 2026;18(1):1-2. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.26.0043
- 925 View
- 22 Download

Guideline
- A practical guide for enteral nutrition from the Korean Society for Parenteral and Enteral Nutrition: Part III. preparation of enteral nutrition formulas
-
In Seok Lee, Ye Rim Chang, Bo-Eun Kim, Youn Soo Cho, Sung-Sik Han, Eunjung Kim, Hyunjung Kim, Jae Hak Kim, Jeong Wook Kim, Sung Shin Kim, Eunhee Kong, Ja Kyung Min, Chi-Min Park, Jeongyun Park, Seungwan Ryu, Kyung Won Seo, Jung Mi Song, Minji Seok, Eun-Mi Seol, Jinhee Yoon, Jeong-Meen Seo, for the KSPEN Enteral Nutrition Committee
- Ann Clin Nutr Metab 2026;18(1):3-9. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.26.0046
-
 Abstract
Abstract
 PDF
PDF - Purpose
This guideline was developed to provide evidence-based recommendations for the safe preparation and handling of enteral nutrition (EN) formulas in order to improve patient safety and promote standardized clinical practice in Korea.
Methods
The key questions addressed the selection of open versus closed feeding systems, the safe preparation and handling of EN formulas, precautions related to blenderized tube feeding (BTF), and essential labeling requirements. Recommendations were drafted and refined through multidisciplinary expert consensus under the auspices of the Korean Society for Parenteral and Enteral Nutrition (KSPEN).
Results
The choice of feeding system should be determined according to the patient’s condition, risk of infection, and anticipated duration of feeding. Closed feeding systems are recommended because they reduce contamination risk and nursing workload, whereas open feeding systems require strict adherence to aseptic technique. For open or reconstituted EN formulas, hang time at room temperature should not exceed 4 hours, whereas closed feeding systems should follow the manufacturer’s recommended hang time. For BTF, administration time should be limited to 2 hours to minimize bacterial growth, and their use is contraindicated in medically unstable or immunocompromised patients. Accurate labeling, including patient identifiers, formula information, administration route, and hang time, is essential to prevent administration errors.
Conclusion
These guidelines provide a practical framework for the safe preparation and management of EN formulas. Adherence to standardized preparation protocols, including appropriate feeding system selection and strict hygiene practices, is essential for reducing complications and improving the safety of EN therapy.
- 1,767 View
- 67 Download
Reviews
- Bedside support for neurologically impaired patients via nutritional evaluations, swallowing function assessments, and gastrointestinal function tests: a narrative review
-
Daisuke Masui
 , Naoki Hashizume, Yoshinori Koga, Hiroto Eto, Hiroki Yoshida, Shotaro Taki, Takato Aikoh, Shiori Tsuruhisa, Tomohiro Kurahachi, Naruki Higashidate, Tatsuru Kaji
, Naoki Hashizume, Yoshinori Koga, Hiroto Eto, Hiroki Yoshida, Shotaro Taki, Takato Aikoh, Shiori Tsuruhisa, Tomohiro Kurahachi, Naruki Higashidate, Tatsuru Kaji - Ann Clin Nutr Metab 2026;18(1):10-17. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0018
-
Abstract
PDF
- Purpose
Neurologically impaired patients often experience complex challenges in respiratory and nutritional management that may necessitate surgical intervention. Furthermore, some patients admitted to specialized facilities for neurologically impaired individuals do not receive adequate postoperative follow-up after being transferred. Kurume University Hospital has established a system of continuous routine rounds at such facilities. This review aims to describe the rationale, methods, and outcomes of multidisciplinary bedside support, with particular emphasis on nutritional evaluation, swallowing function assessment, and gastrointestinal function testing.
Current concept
Routine collaboration between pediatric surgeons and facility-based pediatricians enables continuous perioperative management. Preoperatively, patient background, nutritional status, and family preferences are recorded through structured communication and shared decision-making tools, such as the Ottawa Personal Decision Guide. During hospitalization, multidisciplinary evaluations include bioelectrical impedance analysis for nutritional assessment, endoscopic and pH impedance testing for swallowing function, and multichannel intraluminal impedance monitoring for gastroesophageal reflux. Postoperatively, periodic facility rounds ensure ongoing evaluation, with repeated assessments guiding nutritional optimization, early complication detection, and timely surgical consultation. This approach provides families and healthcare teams with detailed information on functional outcomes, strengthens trust, and enhances continuity of care. Sustained bedside engagement at facilities for neurologically impaired patients improves pre- and postoperative monitoring, promotes seamless collaboration between institutions, and ensures individualized evaluation of nutrition, swallowing, and gastrointestinal function.
Conclusion
By providing actionable data to families and multidisciplinary teams, this model strengthens shared decision-making and supports long-term outcomes. The system may serve as a framework for integrated perioperative care in similar high-risk patient populations.
- 754 View
- 23 Download
- Effectiveness of perioperative rehabilitation and nutrition in esophageal cancer: a narrative review
-
Ryoma Haneda, Yuki Sakai, Kenichi Sekimori, Tomohiro Murakami, Eisuke Booka, Tomohiro Matsumoto, Hirotoshi Kikuchi, Yoshihiro Hiramatsu, Hiroya Takeuchi
- Ann Clin Nutr Metab 2026;18(1):18-26. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0021
-
Abstract
PDF
- Purpose
Esophageal cancer surgery requires robust perioperative management to reduce its high rate of complications. This review evaluates the clinical utility of comprehensive exercise and nutritional therapy, with a specific focus on initiatives led by the multidisciplinary Hamamatsu Perioperative Care Team (HOPE), established at Hamamatsu University Hospital to optimize patient safety and postoperative recovery outcomes.
Current concept
The HOPE protocol involves a diverse team, including surgeons, nurses, pharmacists, and dietitians, who collaboratively implement a multifaceted perioperative care bundle. These interventions include strict smoking cessation, intensive oral care, and immunonutrition incorporating n-3 fatty acids. A distinctive feature of this program is the integration of patient-reported treatment diaries and wearable fitness tracking devices (WFTs) to visualize daily activity, thereby helping to sustain patient motivation. Preoperative rehabilitation focuses on preventing sarcopenia through combined aerobic and resistance training, while postoperative care emphasizes immediate enteral nutrition and early mobilization. Retrospective analyses demonstrated that HOPE implementation reduced Clavien-Dindo grade III or higher infectious complications, pneumonia and surgical site infections, compared with historical controls. In addition, a propensity score–matched analysis showed that WFT users experienced lower pneumonia rates, shorter hospital stays, and better preservation of nutritional markers, including albumin and transthyretin, during the recovery phase compared with non-users.
Conclusion
The HOPE strategy illustrates that combining standard nutritional support and exercise therapy with digital tools enables individualized rehabilitation. This integrated approach reduces morbidity and preserves function, strongly suggesting that incorporation of wearable technology into established surgical care protocols represents a strategy for improving long-term outcomes in high-risk cancer patients.
- 969 View
- 18 Download
Original Articles
- Epigallocatechin gallate increases fatty acid oxidation but not 24-hour survival in lipopolysaccharide-induced endotoxic shock in mice
-
Takayuki Irahara, Ryusuke Katsuki, Dai Oishi, Tsuguaki Terashima, Md. Monirul Islam
 , Umme Salma, Shohag Majumder, Ridwan Ahmed, Eizo Watanabe
, Umme Salma, Shohag Majumder, Ridwan Ahmed, Eizo Watanabe - Ann Clin Nutr Metab 2026;18(1):27-33. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0036
-
 Graphical Abstract
Abstract
PDF
Graphical Abstract
Abstract
PDF - Purpose
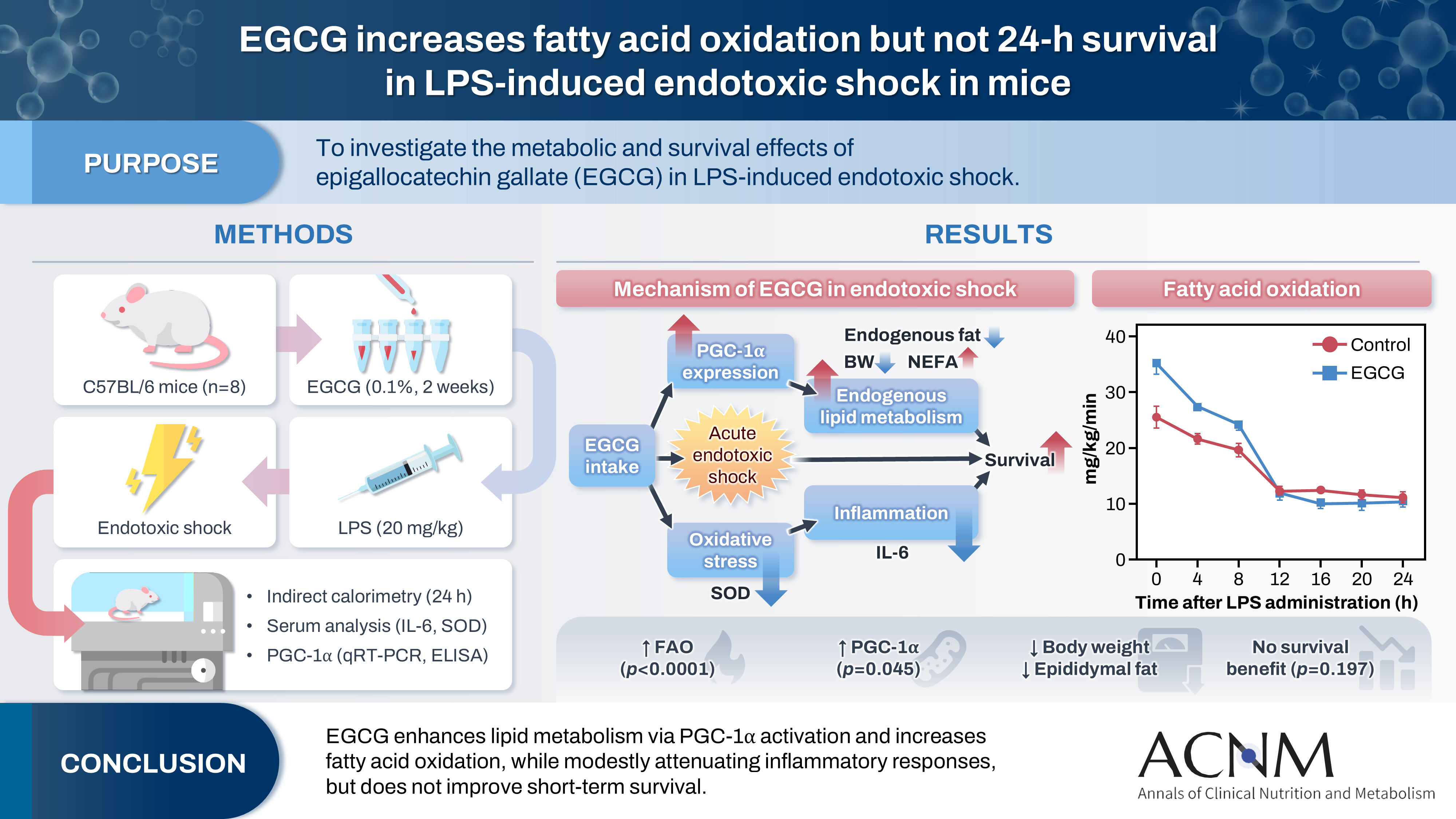
This study aimed to explore the effects of epigallocatechin gallate (EGCG) in critically ill patients using a mouse model.
Methods
C57BL/6 mice were divided into control and EGCG groups (n=8 per group). The EGCG group received a 0.1% EGCG solution for 2 weeks, after which the mice were intraperitoneally injected with a lethal dose of lipopolysaccharide to induce acute endotoxic shock. Indirect calorimetry was performed for 24 hours. Changes in body weight, epididymal fat weight, and survival were measured, together with serum lipid levels, interleukin-6 (IL-6), and superoxide dismutase (SOD) concentrations. The expression of peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC-1α) was determined using quantitative real-time polymerase chain reaction, and its serum concentration was subsequently measured.
Results
Indirect calorimetry showed a significant increase in fatty acid oxidation (P<0.0001) in the EGCG group, along with significant decreases in body weight and epididymal fat weight (P<0.01 and P<0.05, respectively). Survival did not differ significantly between groups (P=0.197). Serum lipid levels, IL-6, and SOD showed numerical differences, although these differences were not statistically significant. Furthermore, hepatic PGC-1α expression showed a tendency toward upregulation, and serum PGC-1α levels were significantly higher (P<0.05).
Conclusion
EGCG stimulates endogenous lipid metabolism through PGC-1α activation and may suppress inflammatory responses; therefore, it may represent a potentially useful nutrient for acute nutritional therapy.
- 2,799 View
- 31 Download
- Association of soy oil-based lipid injectable emulsion with early body weight loss after minimally invasive esophagectomy in Japan: a retrospective cohort study
-
Tomonori Narita, Kazuhiko Fukatsu, Kenichi Kono, Satoshi Murakoshi, Reo Inoue, Midori Noguchi, Nana Matsumoto, Shoh Yajima, Koichi Yagi, Yoshifumi Baba
- Ann Clin Nutr Metab 2026;18(1):34-43. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0030
-
Graphical Abstract
Abstract
PDF
 Supplementary Material
Supplementary Material - Purpose
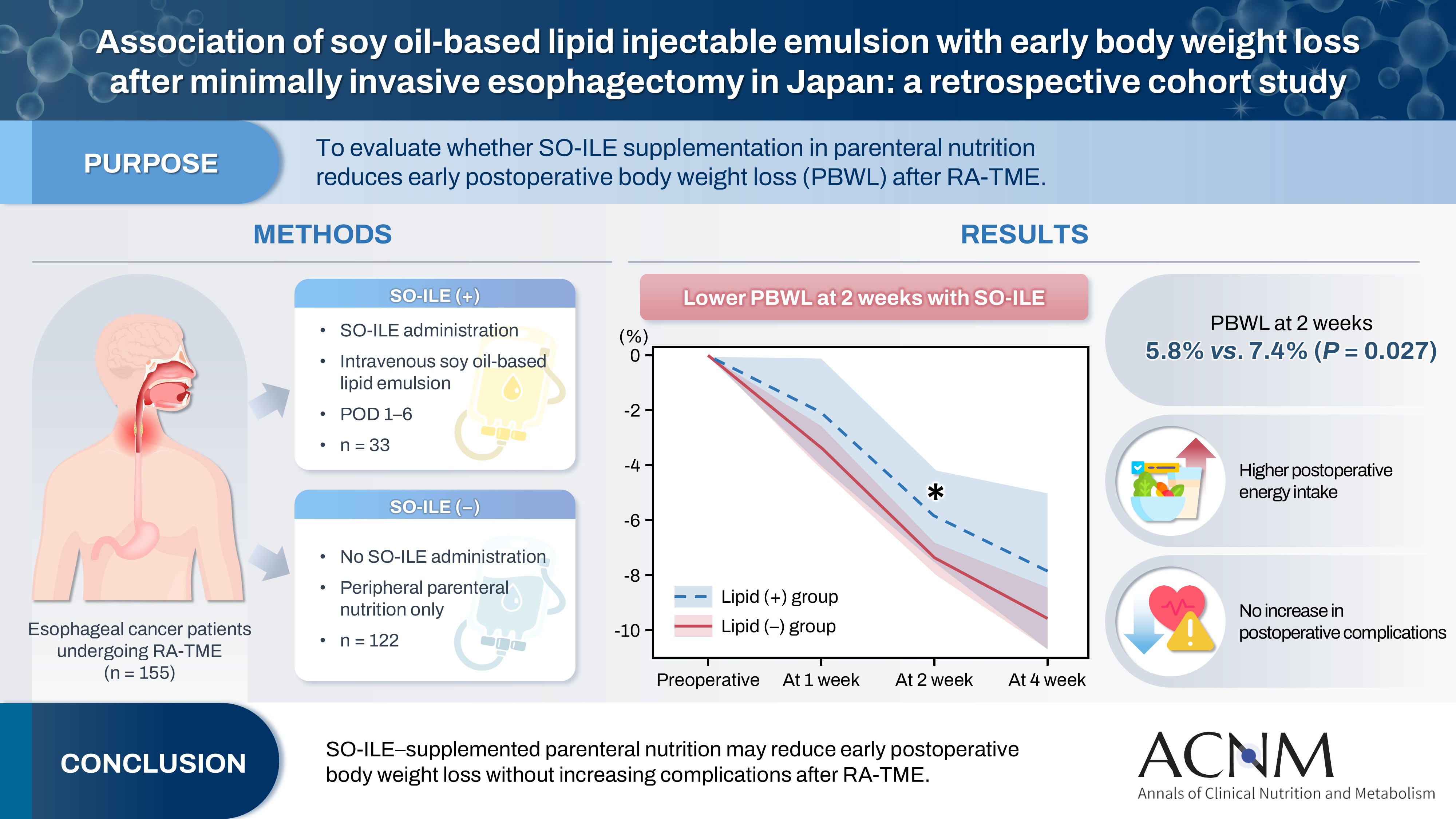
Postoperative body weight loss (PBWL) is associated with poor long-term outcomes following esophagectomy for esophageal cancer, underscoring the critical importance of perioperative nutritional management. Although minimally invasive procedures, such as robot-assisted radical transmediastinal esophagectomy (RA-TME), have become increasingly prevalent, perioperative nutritional strategies have received comparatively limited attention. This study evaluated the impact of soy oil-based injectable lipid emulsion (SO-ILE) on PBWL in patients undergoing RA-TME.
Methods
We retrospectively analyzed 155 patients who underwent RA-TME for esophageal or esophagogastric junction cancer at our hospital between 2011 and 2022. Patients were divided into two groups: the lipid (+) group (n=33), which received SO-ILE between postoperative days 1 and 6, and the lipid (–) group (n=122), which did not receive SO-ILE. Oral or enteral nutrition was withheld until postoperative day 6. Nutrient intake, postoperative outcomes, and nutritional status were compared between the two groups.
Results
Patient backgrounds, surgical outcomes, and postoperative complication rates were similar between the two groups. However, patients in the lipid (+) group received significantly greater total energy and nutrient intake. PBWL at 2 weeks after surgery was significantly lower in the lipid (+) group than in the lipid (–) group (5.8% vs. 7.4%; P=0.027). Univariate analysis showed that absence of SO-ILE administration was the only significant risk factor for PBWL greater than 5% at 2 weeks after RA-TME (P=0.038).
Conclusion
SO-ILE may have the potential to mitigate early PBWL after RA-TME.
- 1,044 View
- 15 Download
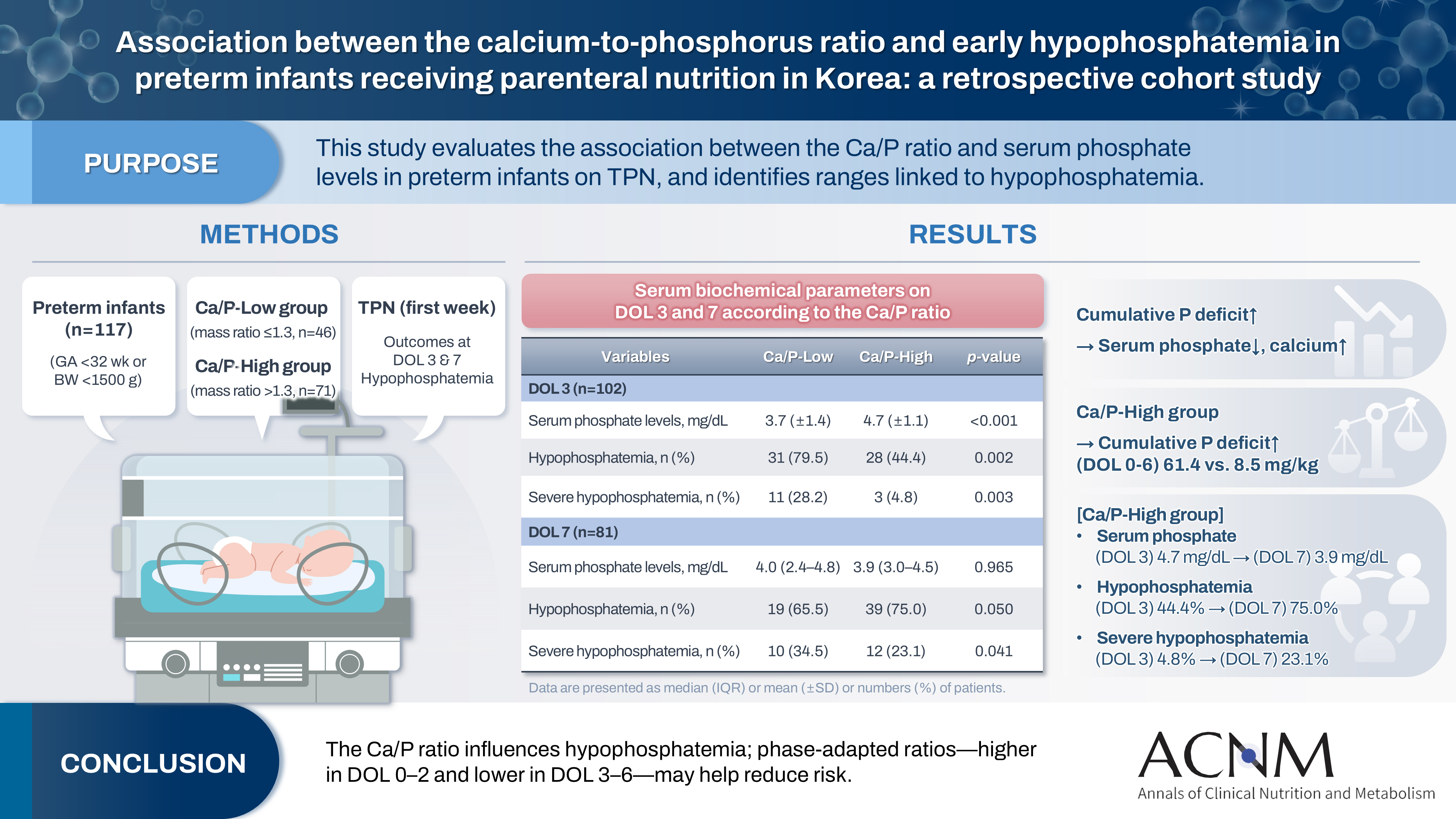
- Association between the calcium-to-phosphorus ratio and early hypophosphatemia in preterm infants receiving parenteral nutrition in Korea: a retrospective cohort study
-
Miseon Han, Jin Ok Kyun, Yoong-A Suh, Jang Hoon Lee
- Ann Clin Nutr Metab 2026;18(1):44-53. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0039
-
Graphical Abstract
Abstract
PDFSupplementary Material
- Purpose
This study aimed to evaluate the association between the calcium-to-phosphorus (Ca/P) ratio and serum phosphate levels in preterm infants receiving total parenteral nutrition (TPN) and to explore Ca/P ratio ranges associated with hypophosphatemia.
Methods
We retrospectively reviewed the medical records of preterm infants admitted to the neonatal intensive care unit at Ajou University Hospital between January 2022 and June 2024. The review focused on TPN composition and serum electrolyte changes during the first week of life. Based on the cumulative Ca/P ratio during this period, infants were categorized into two groups: Ca/P-Low (mass ratio ≤1.3) and Ca/P-High (mass ratio >1.3).
Results
A total of 117 preterm infants were included in the analysis (Ca/P-Low group, n=46; Ca/P-High group, n=71). During the first week of life, the cumulative phosphorus deficit was significantly greater in the Ca/P-High group (61.4 mg/kg vs. 8.5 mg/kg; P<0.001). By day of life (DOL) 7, both hypophosphatemia and severe hypophosphatemia had increased markedly in the Ca/P-High group compared with DOL 3. In the Ca/P-High group, the incidence of hypophosphatemia increased from 44.4% on DOL 3 to 75.0% on DOL 7, while the incidence of severe hypophosphatemia increased from 4.8% to 23.1%.
Conclusion
These findings suggest that parenteral nutrition strategies may benefit from phase-adapted Ca/P ratios rather than a fixed ratio during the first week of life. A higher ratio may be considered during DOL 0–2, whereas a lower ratio may be considered during DOL 3–6, particularly when overall calcium and phosphorus supply is suboptimal.
- 1,383 View
- 28 Download
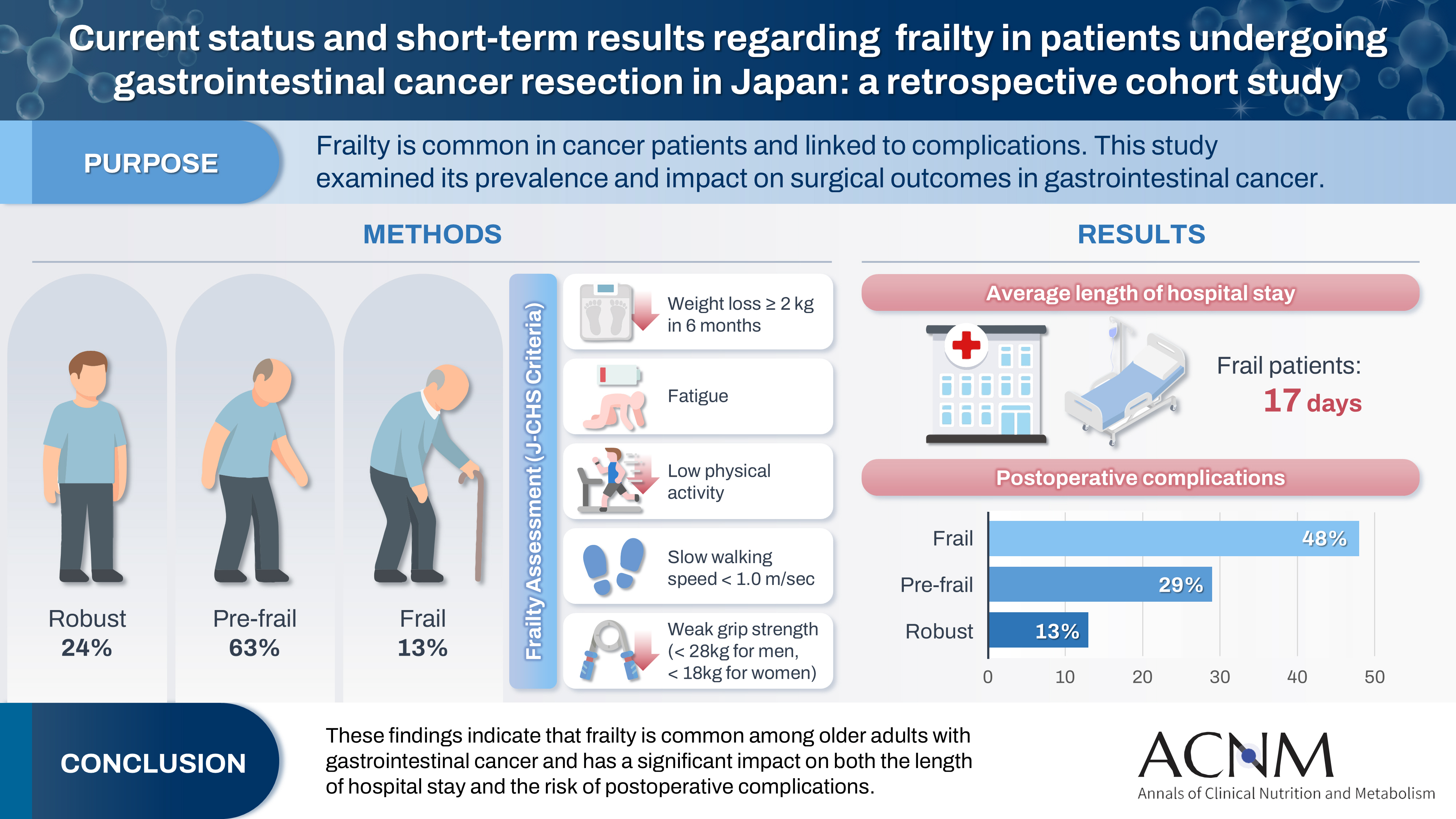
- Current status and short-term results regarding frailty in patients undergoing gastrointestinal cancer resection in Japan: a retrospective cohort study
-
Asuka Yasueda, Junichi Nishimura, Seiji Ikeda, Naotsugu Haraguchi, Hirofumi Akita, Hiroshi Wada, Chu Matsuda, Takeshi Omori, Masayoshi Yasui, Hironari Tamiya, Hideaki Tahara, Hiroshi Miyata
- Ann Clin Nutr Metab 2026;18(1):54-62. Published online March 30, 2026
- DOI: https://doi.org/10.15747/ACNM.25.0013
-
Graphical Abstract
Abstract
PDF
- Purpose
Frailty is a state of physical and cognitive decline that exists between robust health and the need for nursing care. Frailty is reported to occur at a high rate among patients with cancer and is associated with postoperative complications, such as delirium, infection, reduced survival, and rehospitalization. In this study, we investigated the incidence of frailty and surgical outcomes in patients who underwent surgery for gastrointestinal cancer.
Methods
A total of 201 patients who underwent preoperative physical assessment at Osaka International Cancer Institute between July and September 2021 were included. The Japanese version of the Cardiovascular Health Study (J-CHS) index was used to assess the frequency of frailty and related postoperative outcomes.
Results
Among the 201 patients, 27 (13%) were classified as frail and 126 (63%) as pre-frail. Of the 27 frail patients, 22 (81%) were older adults—a significantly higher proportion compared to the pre-frail/robust group (P=0.004). The median hospital stay for frail patients was 17 days (range, 5–98 days), which was significantly longer than that for robust patients (P<0.001). Postoperative complications occurred in 13 frail patients (48%), which was higher than in pre-frail (n=36, 29%) and robust (n=6, 13%) patients. Furthermore, multivariate analysis showed that frailty was an independent risk factor for postoperative complications.
Conclusion
These findings indicate that frailty is common among older adults with gastrointestinal cancer and has a significant impact on both the length of hospital stay and the risk of postoperative complications.
- 876 View
- 12 Download
 First
First Prev
Prev

